
Communication and the impact of stroke
Communication is central to human connection and is often closely tied to one’s identity. Though typically not given a second thought because of its innateness, communication is a complex, multi-step process that relies on domain-general cognition (e.g., attention, memory), language (e.g., semantics, phonology), perception (e.g., hearing, vision), and motor function (e.g., speaking, signing). Successful communication involves integration of information across modalities via neurocognitive and physical processes and thus relies on the functioning and connectivity of many parts of the brain to transform mental representations and sensory input into meaningful communicative actions (for expression/ production) and interpretations (for recognition/ comprehension).1,2
Disruption of any one of these components of communication, due to stroke for example, can result in ineffective or inefficient communication among interlocutors. As such, how disruptions are addressed, such as through intervention, will vary by the communicative component(s) and relevant subcomponent processes affected.
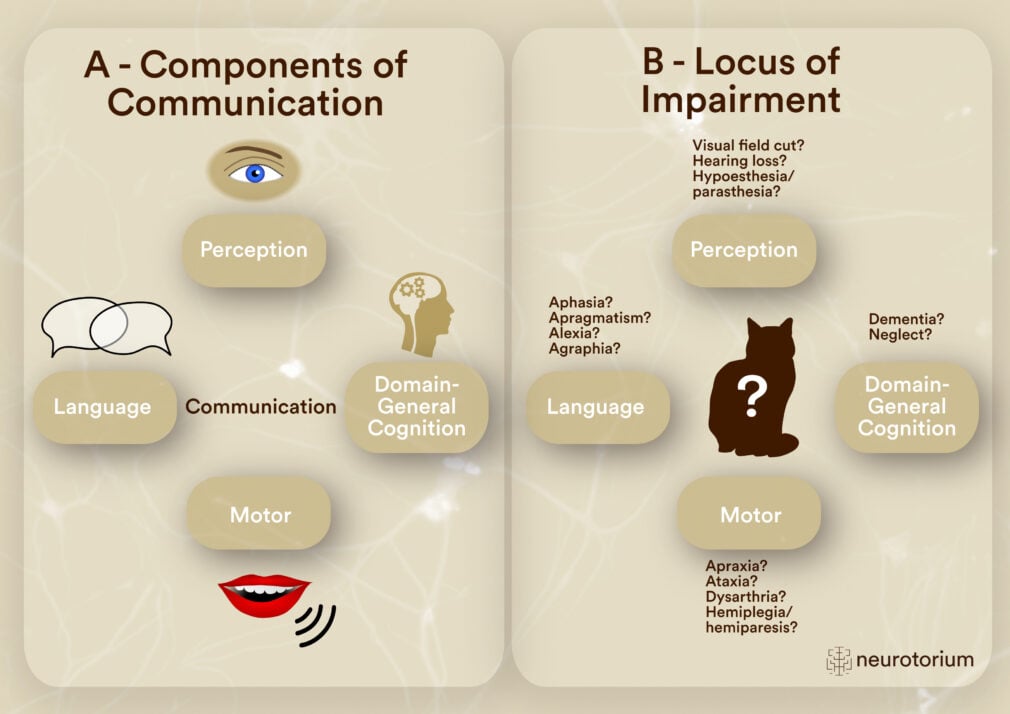
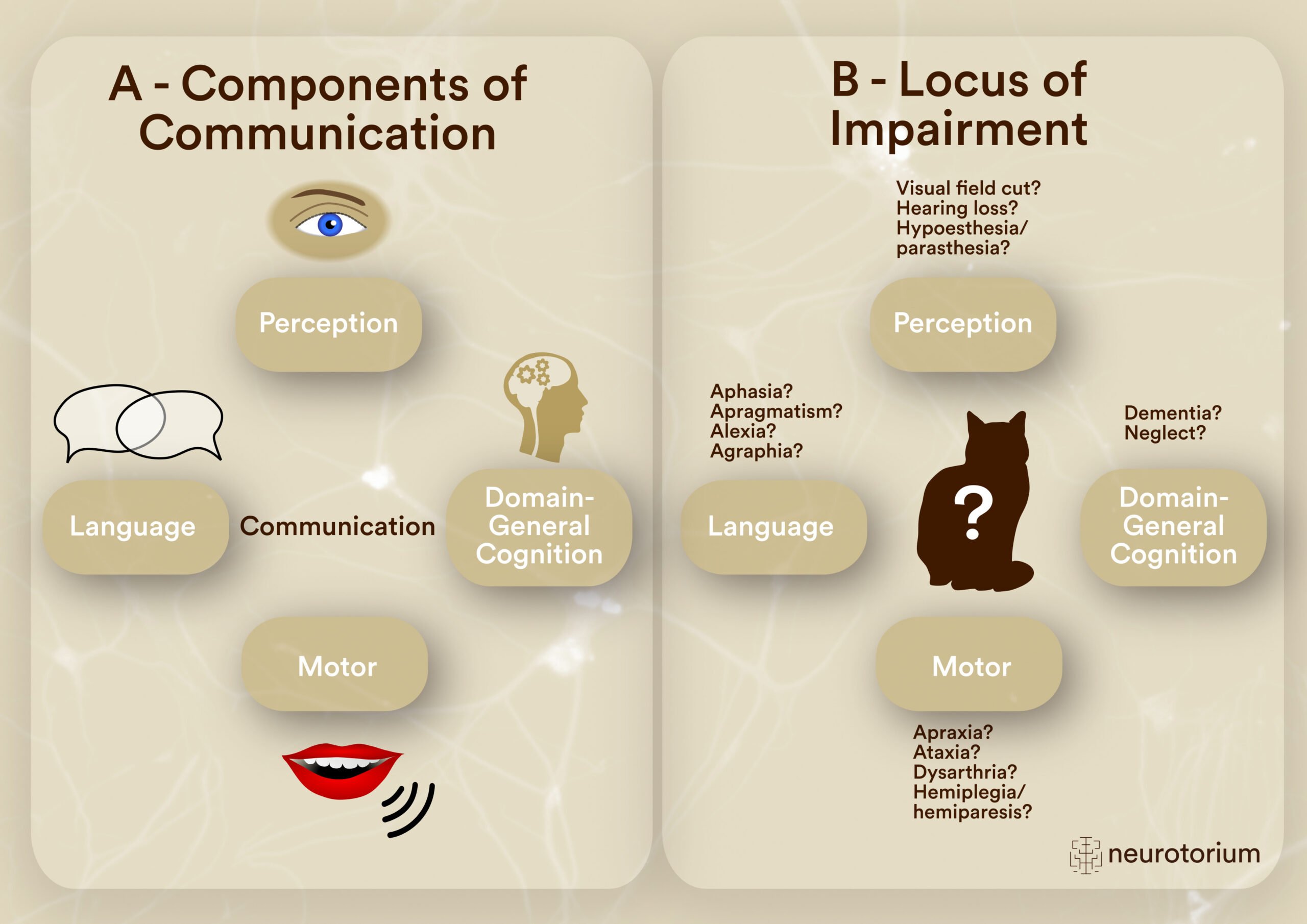
Figure 1: Components needed for a successful communication exchange (A) and possible consequences of disrupted component functioning due to stroke (B)
Part A of the figure highlights the skills necessary to participate in a successful communication exchange with others. (From left, moving clockwise) Language comprises the symbol system that conveys conceptual mental representations into meaningful information to be interpreted by other communication partners. We also need to gather the input from other communication partners via our senses, such as through vision or audition. Domain-general cognitive skills, such as memory and attention, underly our ability to maintain our role as an engaged, active participant in the conversation such as remembering details previously mentioned in the conversation or integrating information from the conversation with prior knowledge. Finally, in order to respond, we rely on motor execution to speak, sign, write, or type in order to send a message to other communicators.
Part B of the figure lists some possible disorders that can occur following acquired impairment or dysfunction at each communication component. Many individuals may present with difficulties recognizing and naming an object, but the locus of impairment, or the underlying cause, of the naming impairment, may differ depending on the component affected. Knowing which component(s) of communication are affected from a stroke through behavioral assessment plays an integral role in determining the course of intervention.
According to the World Stroke Organization,3 a quarter of the world’s population over the age of 25 is expected to suffer a stroke in their lifetime, with over 12 million strokes occurring each year, creating a financial burden of nearly $900 billion in direct and indirect costs internationally. Years of healthy life lost due to stroke-associated disability and death is estimated at over 143 million years, and over 100 million people are living with post-stroke sequelae, including changes to their ability to communicate. At a more personal level, post-stroke communication difficulties can interfere with individuals’ ability to participate fully in their lives, negatively impacting independence,4 relationships,5-8 and quality of life.9
Language and the brain
Theoretical accounts of language processing
Central to communication is language, or the set of agreed-upon symbols that convey meaning. Language comprises the content of messages, which includes semantics (i.e., meaning), as well as the form of these messages, encompassing phonology (i.e., sound system) and morphosyntax (i.e., grammar and sentence structure). Coordination within the language system relies on an unconscious process termed automatic spreading activation,10 wherein activation spreads between and within semantic, lexical, and phonological representations.
Regarding language expression, successful word production relies on spreading activation of conceptual information to the language network, which assists in lexical selection and phonological encoding.11-14
First, a concept (e.g., dog) activates the semantic features of a word (e.g., <furry> <bark/woof> <animal> <tail>). These semantic features in turn activate lexical representations (also referred to as a lemma in some language models)11 onto which phonological representations are encoded (e.g., /dɑg/). This phonological form of the word is then further planned and programmed for motor execution (e.g., articulation, signing) of the word. In a sort of reversal of events, auditory comprehension relies on analysis of acoustic features (e.g., pitch, rhythm, phonetic features [place, manner, voicing]), which follows from the acoustic-mechanical-chemical transduction of the incoming auditory signal completed by the peripheral and central auditory system.15 After acoustic analysis, these representations are mapped onto phonological-lexical representations which then activate corresponding semantic representations for comprehension.15,16 Comprehension and production at the single word level is embedded within more complex linguistic structures, like sentences, which requires planning at the message (conceptual form of sentence), functional (predicate-argument structure), and positional (surface sentence structure) levels prior to motor execution of the message.15,17 Finally, the combination of sentences into discourse-level language processing incorporates not only these microlinguistic processes mentioned but also macrostructural processes,15,18 including how well ideas connect across sentences (cohesion), connect to the main idea or gist of the discourse topic (coherence), and disambiguate and integrate information shared in the communicative exchange.
Regarding language expression, successful word production relies on spreading activation of conceptual information to the language network, which assists in lexical selection and phonological encoding.11-14
In addition to form and content, the manner or use of language, termed pragmatics, is vital to a message’s meaning, especially when the words of a message contradict or are incongruous with the intended meaning, such as with sarcasm. Language use can be influenced by context,19 requiring individuals to code-switch depending on the social situation and/or interlocuters engaged. Consider, for example, the manner in which you speak to a group of friends at a bar versus a group of coworkers (including your manager) during a meeting and how context constrains language use.
Language use can be influenced by context,19 requiring individuals to code-switch depending on the social situation and/or interlocuters engaged.
In this video, Alexandra Z Durfee, Ph.D., discusses aphasia, a language disorder often resulting from left-hemisphere strokes, causing challenges with speaking, listening, reading, and writing.
Alexandra Z Durfee, Ph.D. also discusses the consequences of right hemisphere strokes while introducing apragmatism and highlighting the difficulties people face with non-literal language and emotional expression post-stroke.
Neuroanatomical correlates of language
The notion that different parts of the brain, including whole hemispheres (lateralization) or specific structures (localization), are specialized for varying functions, like language, is not novel. Leading theories and empirical evidence of language processing, particularly the microlinguistic elements of language, in the brain have recently focused on a dual stream architecture recruiting more of the left cerebral hemisphere (as compared to the right cerebral hemisphere) for processing. In Hickok and Poeppel’s model,2,20 spectrotemporal analysis of the incoming auditory stimulus is first processed in the superior temporal gyrus and then phonologically decoded around the superior temporal sulcus.
Leading theories and empirical evidence of language processing, particularly the microlinguistic elements of language, in the brain have recently focused on a dual stream architecture recruiting more of the left cerebral hemisphere (as compared to the right cerebral hemisphere) for processing.
Further processing by ventral structures supports sound-to-meaning mapping, or more comprehension and meaning-based processes, while recruitment of more dorsally-situated structures supports sound-to-motor, or more production-based processes. The bidirectionality included in the dual stream model highlights that this network is critical for language and is not modality- (reading vs. listening vs. speaking) or task- (naming vs. repetition) specific. Additional support for dual stream language processing in the right hemisphere is observed as well but within the context of recognition and expression of emotions conveyed through tone of voice or vocal inflection, termed emotional (affective) prosody at this time.21,24
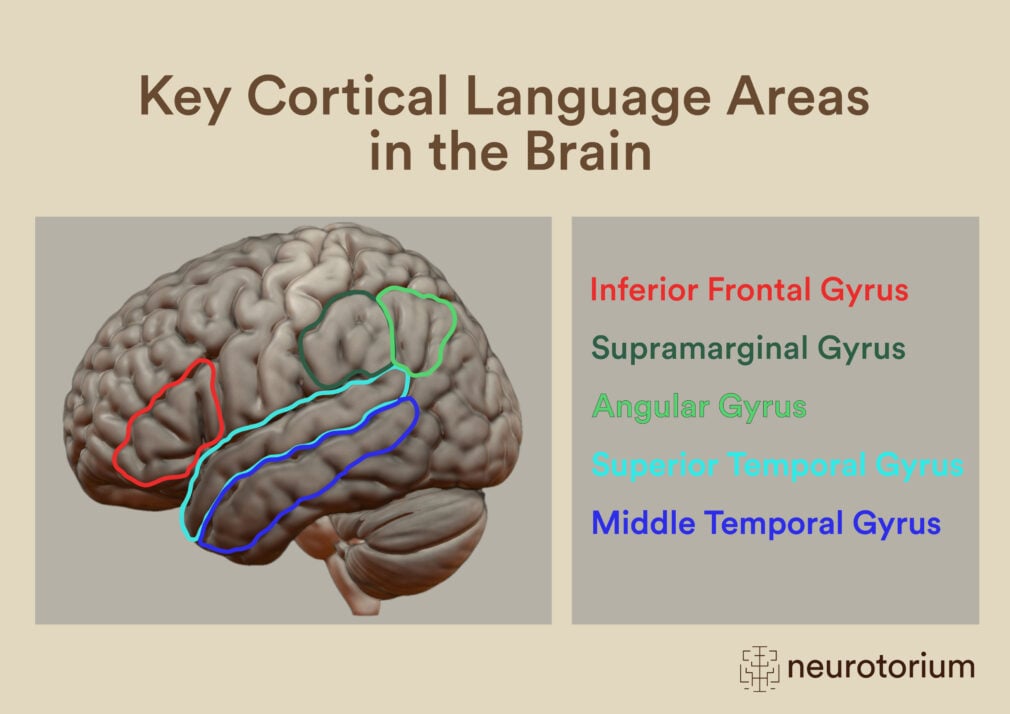
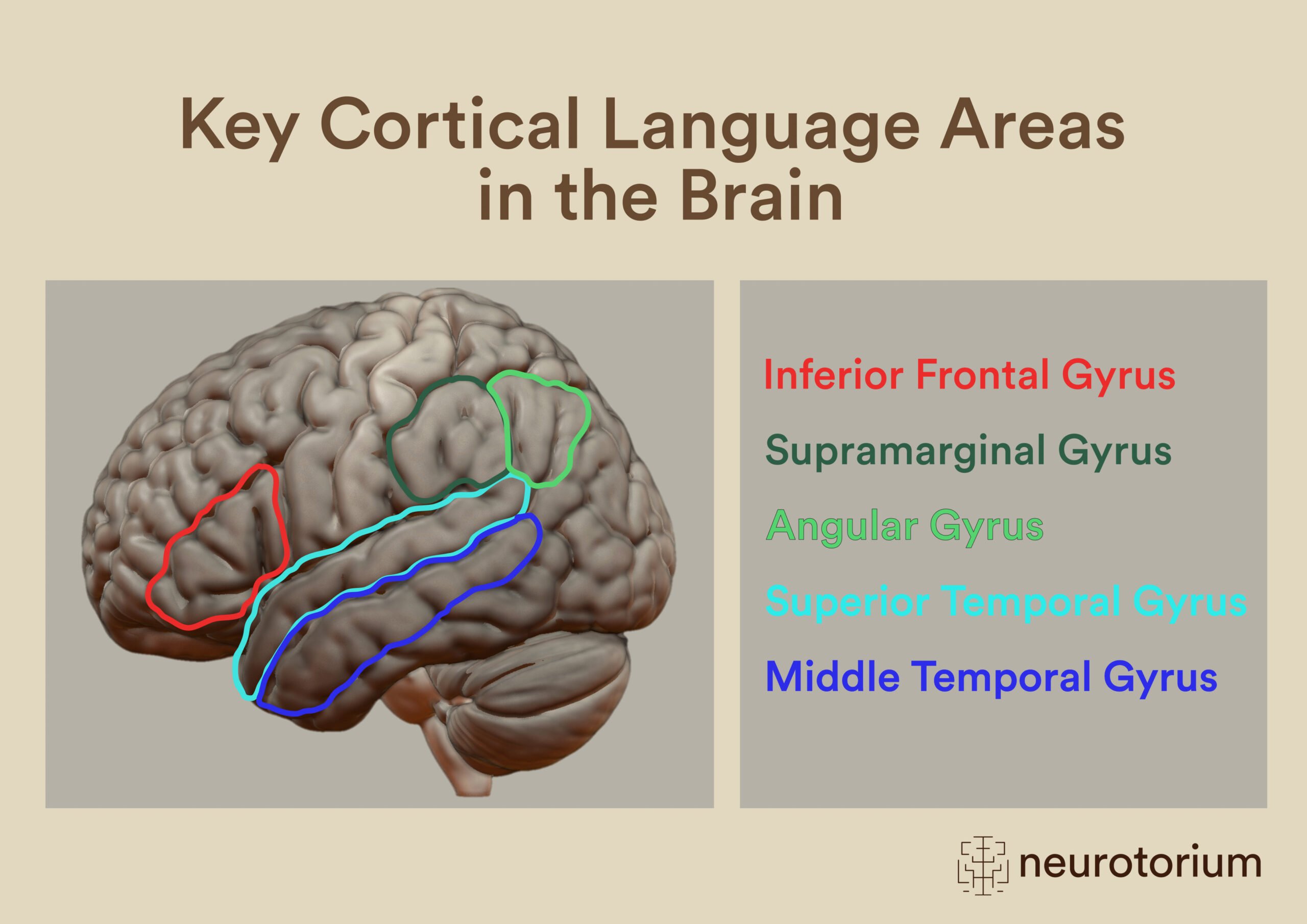
Figure 2: Key Cortical Language Areas in the Brain
There are several critical cortical regions in the frontal (red tones), parietal (green tones), and temporal (blue tones) lobes of the brain that support language processing. Growing evidence point to similar activated regions in right hemisphere homologues not shown here. These highlighted language regions don’t work in isolation but rather are supported by activity in other cortical and subcortical regions that assist with further sensory, motor, and association/integration processes. Association fibers connecting cortical language hubs include the uncinate, arcuate (superior longitudinal), inferior fronto-occipital, and inferior longitudinal fasciculi.81-85
Not only are cortical gray matter structures critical in language processing but so are the associative (intra-hemispheric; e.g., arcuate fasciculus), commissural (inter-hemispheric; e.g., corpus callosum), and projection (cortico-fugal/-pedal; e.g., thalamocortical radiations) white matter tracts that connect them, as disconnection of white matter tracts can also contribute to language issues.23,25 Additionally, there is evidence for subcortical aphasias26-28 as well as for language processing changes following some cerebellar strokes.29 A final consideration to note is the influence of dysfunctional rather than damaged tissue especially during the early acute stages of stroke recovery. In contrast with damaged tissue that is not functional because of the stroke, dysfunctional tissue is not yet functioning at full capacity due to a reduction in blood flow. Once blood flow is re-established to dysfunctional tissue, behavioral performance improvements have been observed.30,31
An understanding of the theoretical, cognitive, and neuroanatomical underpinnings of language help to contextualize the types of errors observed when there is damage to the language network that causes subsequent communication deficits and are critical in determining how to address those deficits with targeted intervention.
Post-stroke language Impairments: Characteristics
Aphasia
For most people when a stroke occurs to the left hemisphere of the brain, the resultant language impairments are called aphasia. Aphasia impacts functional language use in communication, and roughly a third of individuals who sustain a left hemisphere stroke will demonstrate aphasia after their hospitalization.15 Networks of the microlinguistic elements of language as previously mentioned (i.e., semantics, phonology, morphology, syntax) are negatively impacted in aphasia, which can result in impairments of auditory and reading comprehension as well as spoken and written language use. Even though general cognitive changes are observed in aphasia,32-34 the acquired disorder is emphasized as a loss or impairment of language and not intellect.
Aphasia impacts functional language use in communication, and roughly a third of individuals who sustain a left hemisphere stroke will demonstrate aphasia after their hospitalization.15
Depending on the pattern of language difficulties observed, aphasias can be further classified into different subtypes. These cortical aphasia subtypes (e.g., Broca’s aphasia, transcortical sensory aphasia) take into consideration relative preservation and relative impairment of verbal fluency, auditory comprehension, and repetition skills. Impaired naming or lexical retrieval, termed anomia, is a pervasive symptom reported across aphasias and is thus not as useful as the other language skills to differentiate subtypes. One benefit of this aphasia classification system is shared terminology use among clinicians, primarily speech-language pathologists (speech therapists), to support continuity of care. However, the system falls short of defining what relative preservation, as compared to impairment, of a skill is, especially in cases that do not neatly demonstrate total impairment of a skill (e.g., auditory comprehension), and the tasks chosen to assess language can influence performance (e.g., such as in discourse production).35,36 As a result, aphasia subtypes (e.g., all Broca’s aphasias) are not a homogenous group in terms of language characteristics and lesion locations. Additionally, aphasia classification methods may not be as sensitive to language changes evident in discourse.37 Because of these gaps, incorporating use of network-based approaches, such as that posed by the dual stream model of language,2,20 and model-based approaches, such as for word retrieval11-14 or auditory comprehension,15,16 is critical to understand the relationship between intact and impaired language modalities as well to identify the underlying cause(s) of observed language deficits.
| Aphasia Subtype | Fluency | Auditory
Comprehension |
Repetition |
| Global | Nonfluent | – | – |
| Mixed transcortical | Nonfluent | – | + |
| Broca’s | Nonfluent | + | – |
| Transcortical motor | Nonfluent | + | + |
| Wernicke’s | Fluent | – | – |
| Transcortical sensory | Fluent | – | + |
| Conduction | Fluent | + | – |
| Anomic | Fluent | + | + |
Table 1: Cortical Aphasia Subtypes
This diagram represents the traditional classification schemes for cortical aphasias that use fluency (verbal output), auditory comprehension, and repetition skills as methods to triage people into different aphasia subtypes. A plus (+) represents a relative strength or preservation of skill post-stroke while a negative (-) represents a relative weakness or impairment of skill post-stroke.
Apragmatism
Historically, language/communication changes following right hemisphere stroke have been referred to by many names – non-aphasic language disorder, pragmatic aphasia, and more recently as cognitive-communication disorders.38 Though the names envelop the observed changes, the lack of a consistent label introduces bias and hurdles into clinical and research efforts.38 Clinically, continuity of care may be compromised for these individuals. Many adults following a right hemisphere stroke are likely not referred for appropriate evaluation by a speech-language pathologist39 even though studies suggest a non-trivial incidence and prevalence of communication-specific issues.40-42 Additionally, recent surveys conducted in the United States and Australia revealed that many speech-language pathologists feel ill-equipped to address (including assessment and treatment) right hemisphere stroke communication needs43 and call for priorities in communication assessment development.44 In research, an inconsistent label renders large-scale systematic literature reviews an even more laborious process.
Many adults following a right hemisphere stroke are likely not referred for appropriate evaluation by a speech-language pathologist39 even though studies suggest a non-trivial incidence and prevalence of communication-specific issues.40-42
Because of these challenges noted, recent efforts by a group of researchers who formed the International Right Hemisphere Collaborative have focused on redefining the term Apragmatism, first used by Penny Myers,45 to describe the constellation of communication changes observed following right hemisphere damage.38 Centered on the idea of pragmatics, or appropriate language use, disruptions to communication are embedded within discourse and are often associated with macrolinguistic issues, or issues interpreting or presenting contextually appropriate or intended meaning, rather than the microlinguistic difficulties observed in aphasia.
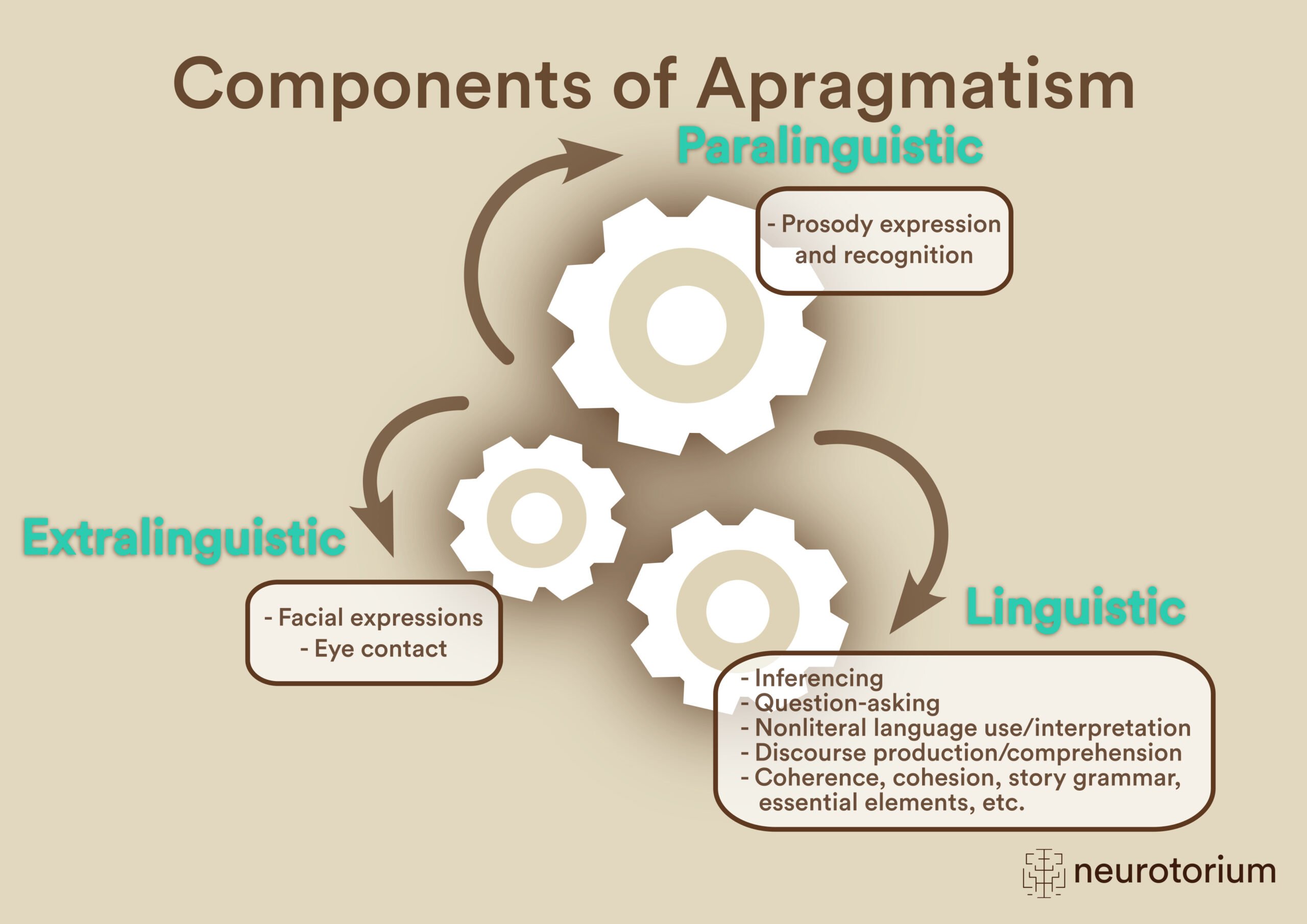
Apragmatism comprises three components – linguistic, paralinguistic, and extralinguistic.38 Disturbances may be seen in a single component or across multiple components and can impact expression and comprehension processes. The linguistic component of apragmatism comprises the appropriate use or comprehension of language. Discourse characteristics of individuals with linguistic component difficulties include verbosity, tangentiality, disorganization (including poor coherence and cohesion), or paucity of speech.46,47 Individuals may struggle with inferencing,48-50 question-asking,51 nonliteral language,52 and referential language (e.g., anaphora, determiner use in English).53-55 The paralinguistic component consists of the appropriate use or understanding of prosody, or vocal inflection through manipulations of pitch, speech rate, rhythm, and volume. Paralinguistic impairments are most often seen in emotional (affective) prosody recognition56 but are also common for emotional prosody expression57-60 and may also occur with linguistic prosody (including grammatical [e.g., prosodic pattern for statement versus a question], lexical [e.g., record versus record], and pragmatic [i.e., prosodic pattern used to emphasize/highlight specific information; I thought you were picking up the cake? vs. I thought you were picking up the cake?]).61 The final component, extralinguistic, includes the behaviors or rules that guide language use, including facial expressions62,63 and conversational turn-taking rules/cues.64
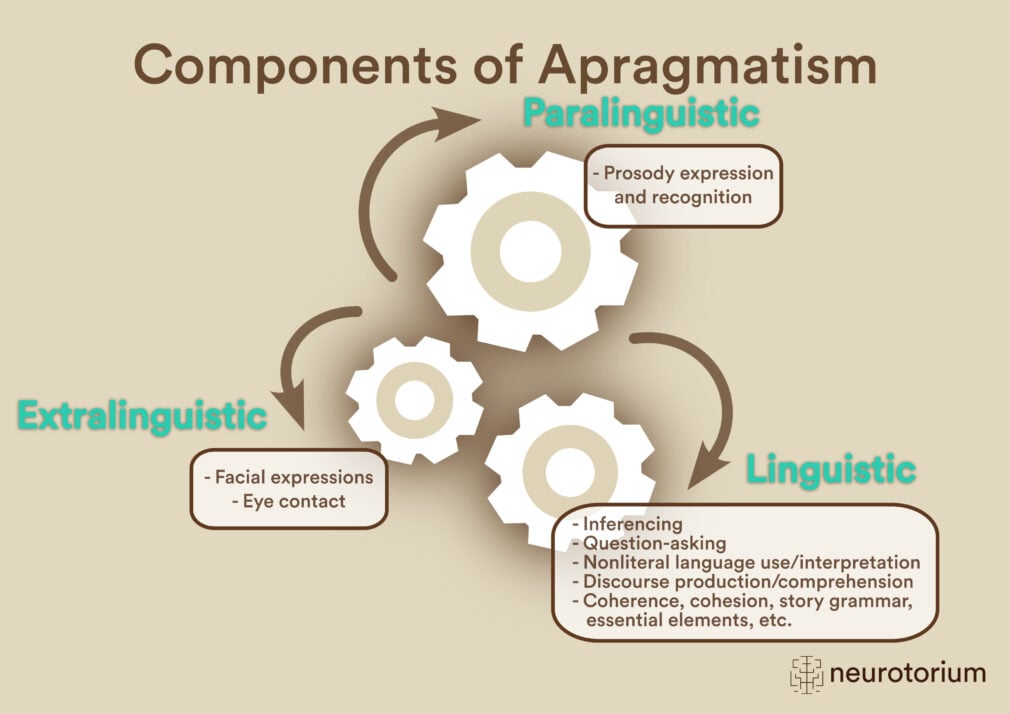
Figure 3: Components of Apragmatism
Apragmatism is a new term used to describe the communication-specific changes that occur as a result of acquired right hemisphere brain damage, such as from stroke. The term was first introduced by Peggy Myers (2001)87 and has been specified more recently by a group of researchers in acquired right hemisphere cognitive-communication disorders.88 Apragmatism comprises paralinguistic, extralinguistic, and linguistic components that may be impacted due to a right hemisphere stroke.
Post-stroke language impairments: Treatment
Treatment for post-stroke language impairments is primarily behavioral and led by a speech-language pathologist following comprehensive evaluation. Broadly speaking, behavioral interventions focus on restitution (i.e., strengthening or relearning of the impaired language process) or compensation (i.e., learning a new skill or way to circumvent the impaired language process) such as life participation approaches that include a critical, holistic lens on how to improve one’s quality of life with a stroke-induced language impairment such as through use of frame proposed by the World Health Organization International Classification of Functioning, Disability, and Health.6,65 There are many different behavioral intervention approaches published for aphasia,66,67 and more research is starting to elucidate what approaches may be better than others based on individual characteristics.68-72 Unfortunately, whilst there are published behavioral interventions for apragmatism43,73 (for recent reviews, see74-76) these are far fewer than what exist for aphasia; however, research in this area continues to grow. Promising behavioral intervention adjuvants, including noninvasive brain stimulation77,78 virtual reality,79 and pharmacological therapies,80 are currently being explored.
In this video, Alexandra Z Durfee, Ph.D., discusses the role of language and breaks down communication into its core components: exchanging ideas, the symbols (words) we use, their sounds, and sentence construction while highlighting the importance of motor skills for speaking or signing, and cognitive skills such as memory and attention.
Related content
Lacunar infarctions are small subcortical infarcts, <1.5 cm in diameter, within deep areas of the brain
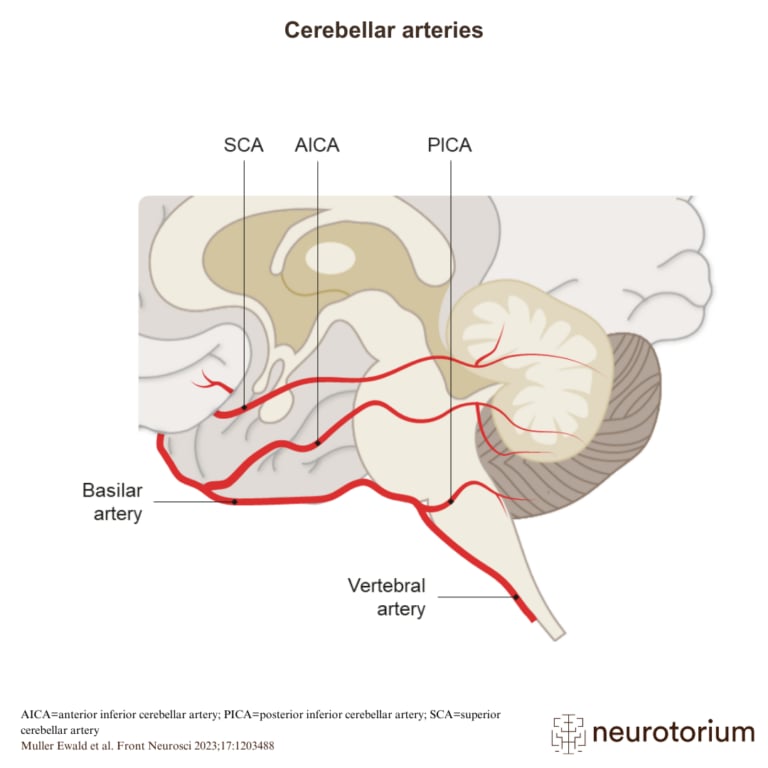
The cerebellum is supplied with blood via three branches of the basilar artery – the posterior inferior cerebellar artery (PICA), the anterior inferior cerebellar artery (AICA), and the superior cerebellar artery (SCA).
{kind=link}
{kind=link}
{kind=link}
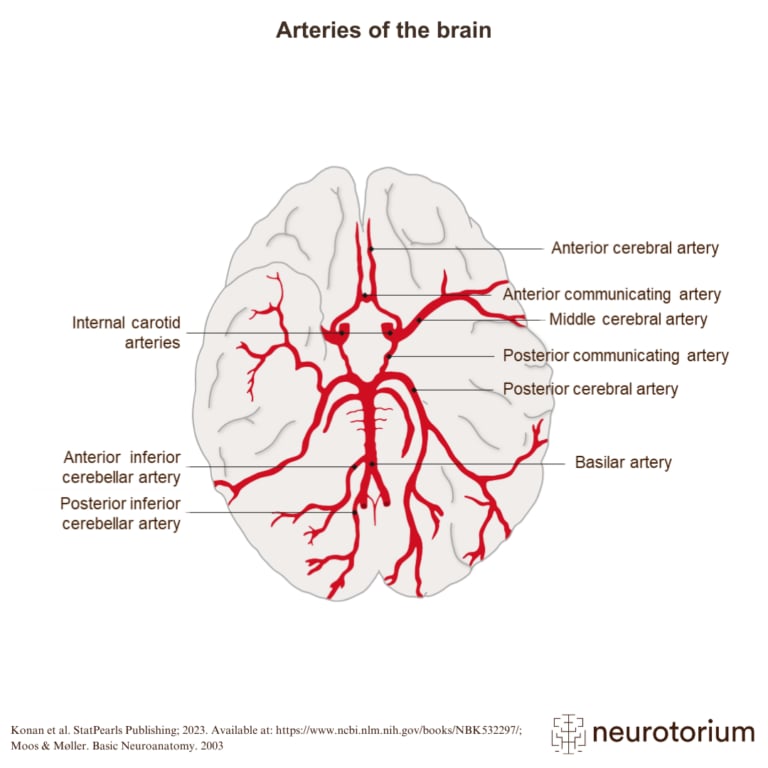
The image shows how the blood supply of the brain is arranged.