Slide Decks on Migraine
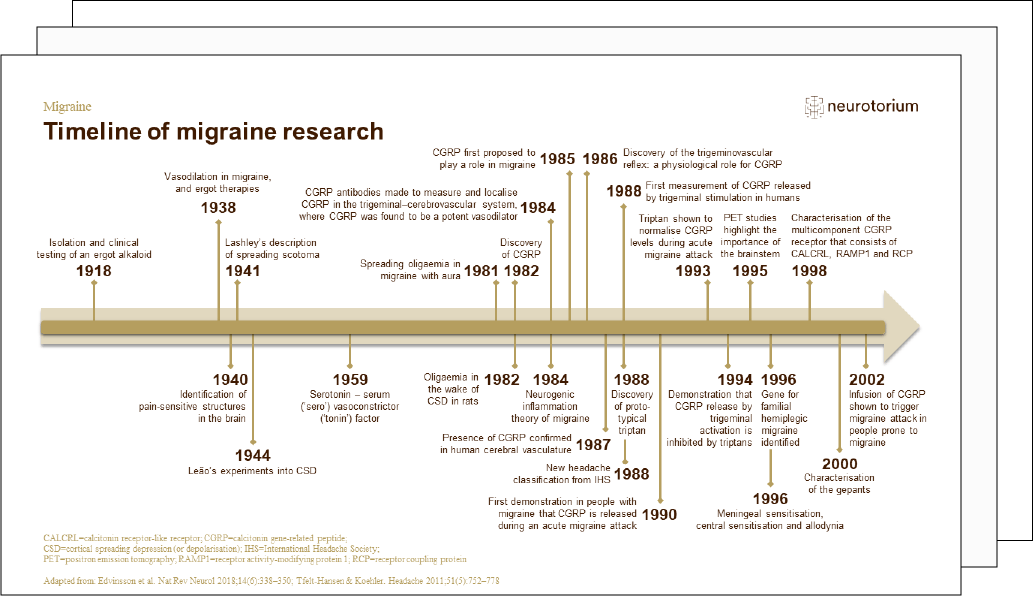
Migraine is a chronic neurological disease characterised by episodic attacks of head pain. It is a burdensome condition and one of the commonest neurological diseases worldwide.
Get an introduction to what is currently known about migraine by going through our slide decks. You can scroll through the slides, read the presenter notes or download the slides and use them for your own presentations.
Would you like to know what triggers migraine attacks?
History, Definitions, and Diagnosis
The perception of migraine has changed substantially through the last century. This slide deck explores basic migraine concepts and definitions. Go to the slide deck.
Epidemiology and Burden
This slide deck describes current knowledge on the economic and general burden of migraine. You will also find a brief introduction to the risk factors for the onset of migraine. Go to the slide deck.
Neurobiology and Aetiology
This slide deck offers insight into the neurobiology and aetiology of migraine and discusses pain and nociception, the pathology of migraine and the brain regions involved in migraine. Go to the slide deck.
Course, Natural History, and Prognosis
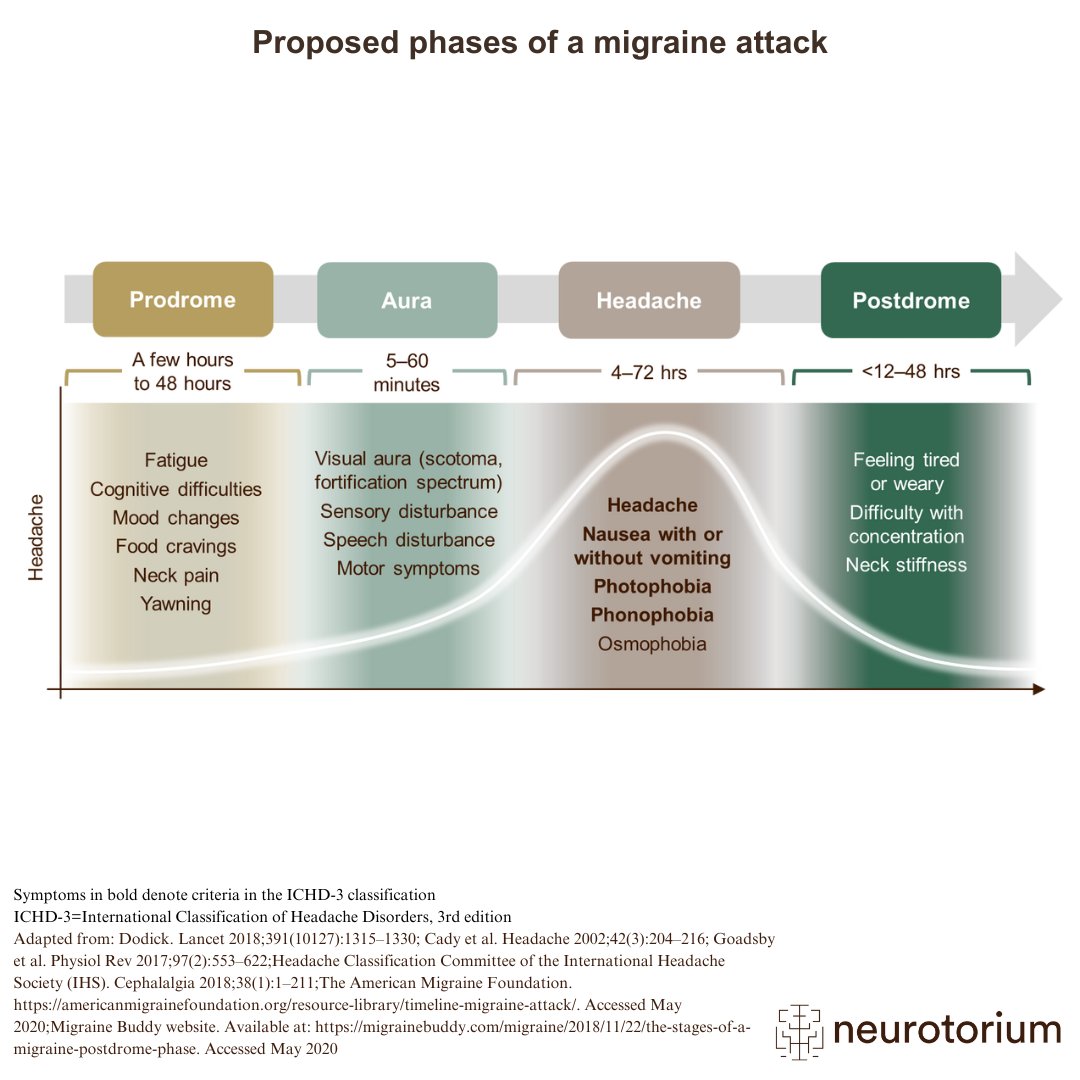
In this slide deck you will find descriptions and illustrations of migraine attacks and triggers, including the four phases of a migraine attack. The slide deck also outlines the evolution of migraine from episodic to chronic and gives an introduction to migraine prognosis. Go to the slide deck.
Comorbidities
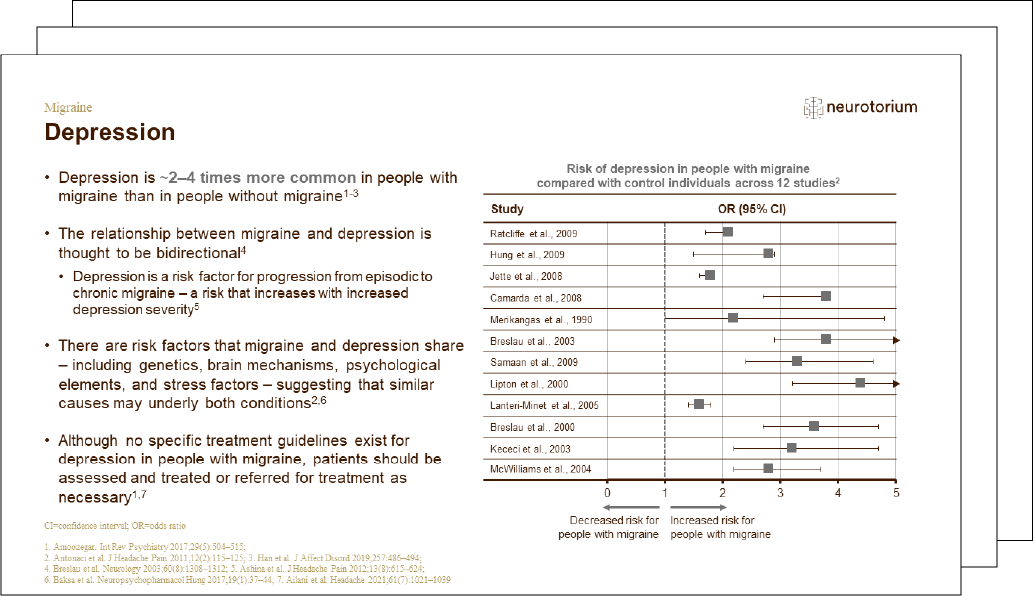
Determining the relationship between migraine and a comorbid condition is complicated. This slide deck discusses in detail the presence of comorbidity in Migraine.
Treatment Principles
In this slide deck you will find basic concepts and definitions related to modern treatment approaches such as the use of analgesics and NSAIDs, as well as more targeted therapies, such as triptans and CGRP medications. Go to the slide deck.
Articles on Migraine
Migraine is a prevalent neurological disorder characterized by recurrent and disabling attacks of moderate to severe headache. Migraine attacks are triggerable, a feature systematically investigated in human models of migraine.
- Human Models of Migraine and Scientific Advances in Migraine Treatments
 Migraine is a prevalent neurological disorder characterized by recurrent and disabling attacks of moderate to severe headache
Migraine is a prevalent neurological disorder characterized by recurrent and disabling attacks of moderate to severe headache
Download Illustrations & Figures on Migraine
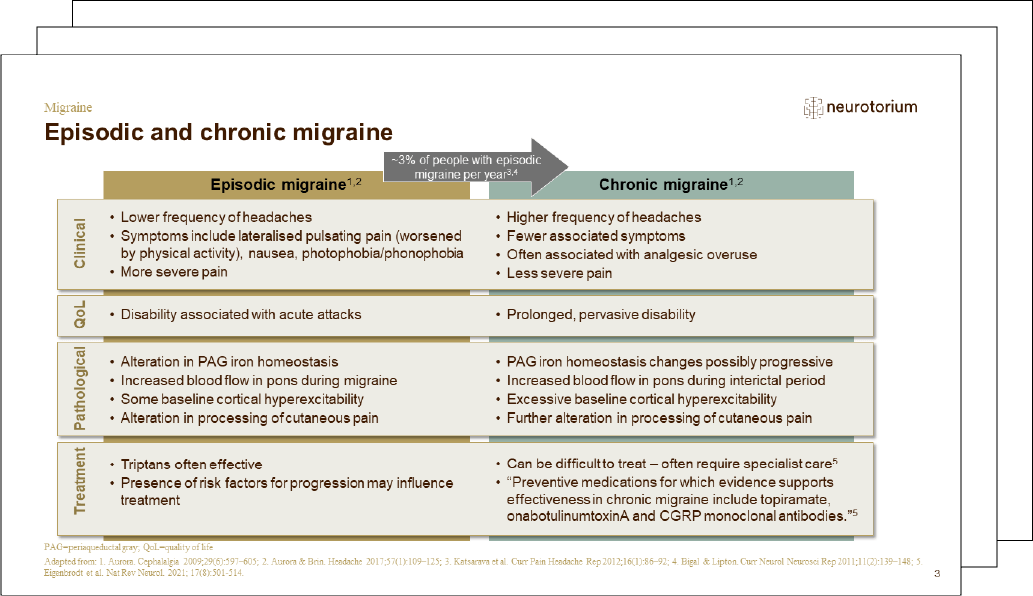
Migraine is a complex spectrum disorder. The differences between people with episodic and chronic migraine highlight the need for treatments to be tailored to each group. Browse our library of downloadable psychiatry and neurology illustrations – everything you need for your presentations. This resource includes illustrations and figures on a range of key concepts or neuroscience facts.
Watch the Videos on Migraine
Professors Lars Edvinsson, Peter Goadsby, Michael Moskowitz and Jes Olesen were awarded The Brian Prize in 2021 for their outstanding research on the causes and treatment of migraine.
Neurotorium and The Brain Prize partners have made educational resources on the winning topic available to all who are interested in learning more. You can read about the award-winning research on migraine at The Brain Prize website.
The Brain Prize Explainer – Migraine
In this documentary film, developed by the team behind The Brain Prize at the Lundbeck Foundation, you can learn more about migraine and the research that led to the brain prize in 2021, and you hear from a patient who suffers from the rarer condition of chronic migraine.
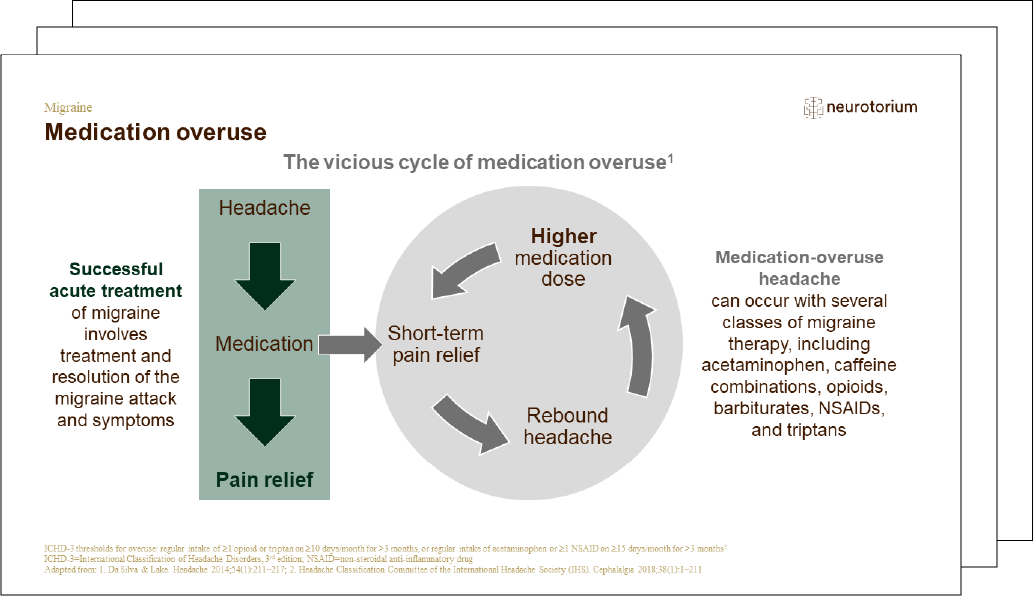
Understanding Medication Overuse Headaches
In this video, Professor Messoud Ashina discusses the importance of proper diagnosis in migraine treatment, distinguishing between primary and secondary headaches.

Human Models of Migraine
In this video, Rune Häckert Christensen, MD, PhD-fellow discusses how human models of migraine have identified key molecular triggers like CGRP and PACAP, leading to a revolution in treatment.
Frequently Asked Questions (FAQ)
The information provided in this document is for educational purposes only and is not a substitute for medical care. If you have questions about your health, speak with a healthcare professional.
Migraine is a brain disorder that characterized by recurrent headache attacks, often accompanied by other neurological symptoms. Migraine comes in two main forms:
(1) Migraine without aura: The most common type. The headache phase is experienced without aura symptoms.
(2) Migraine with aura: About one in four people with migraine have an aura – typically a temporary visual disturbance – before the headache begins.
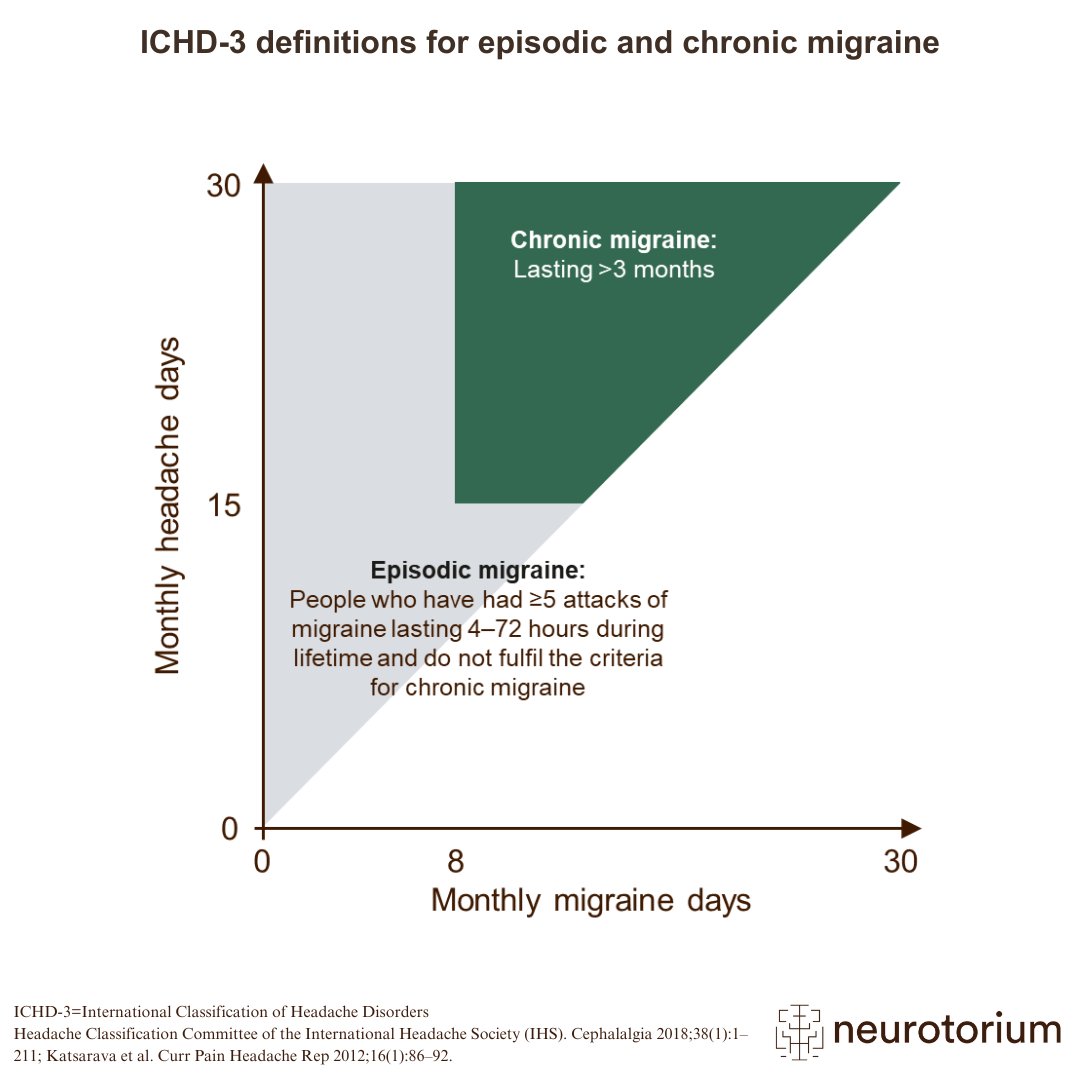
Migraine can be described further based on how often headaches occur. Episodic migraine occurs up to 14 headache days in a month. Chronic migraine is characterised by 15 or more headache days in a month, with at least eight of them fitting migraine criteria.
Migraine is not just a “bad headache.” In addition to severe head pain, attacks are often associated with nausea and vomiting, increased sensitivity to light, sound, or smells, and can be disabling – making it hard to carry out daily activities during an attack.
References
Although we do not know the exact cause of migraine, researchers have found several common triggers, grouped into four main categories.
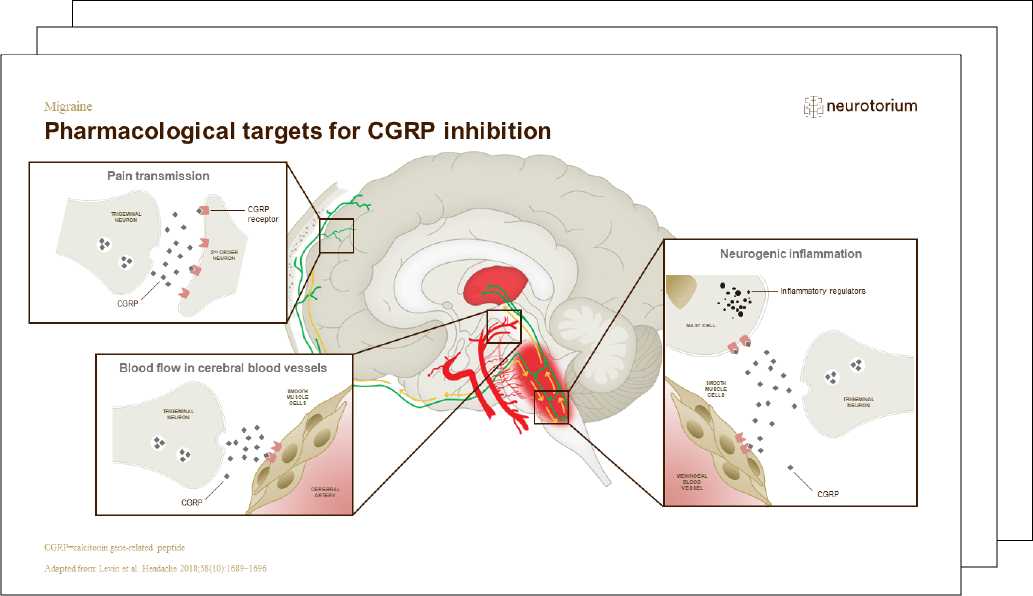
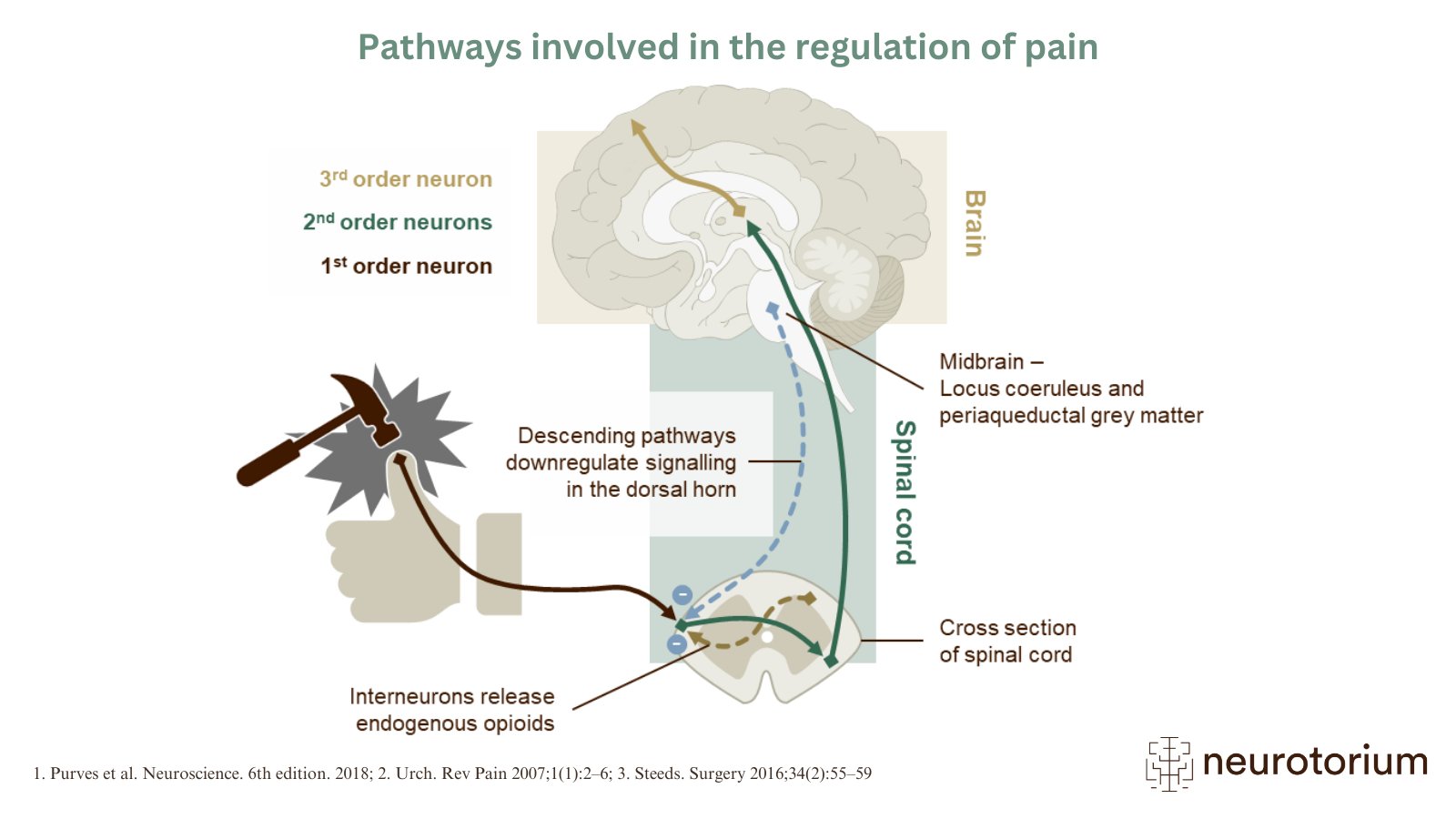
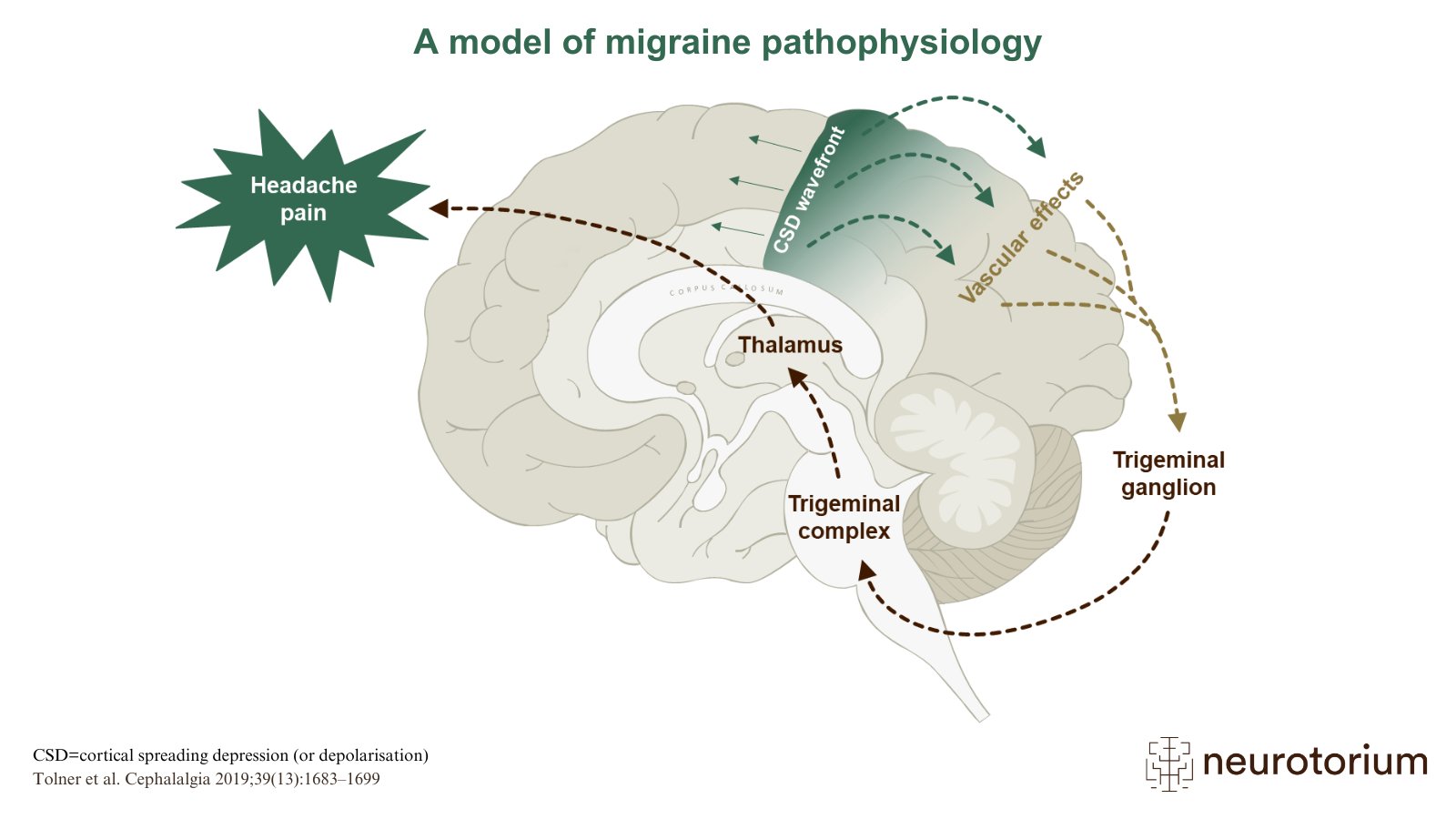
The brain is covered by protective layers called the meninges, which contain many blood vessels. Nerve fibers run alongside these vessels and play an important role in pain signaling. A migraine attack is thought to begin when these nerve cells become unusually active and start sending repeated pain signals.
In response, these nerve cells release substances that cause nearby blood vessels to widen and remain active, which helps maintain the pain. These signals are then transmitted to the brain, leading not only to headache but also to symptoms such as nausea and sensitivity to light and sound.
People differ in how sensitive they are to factors that can trigger migraine. For some, relatively minor changes such as bright light or slight disturbances in sleep can be enough to provoke an attack, while others require stronger triggers. This variation helps explain why migraine occurs more frequently in some individuals than in others.
References
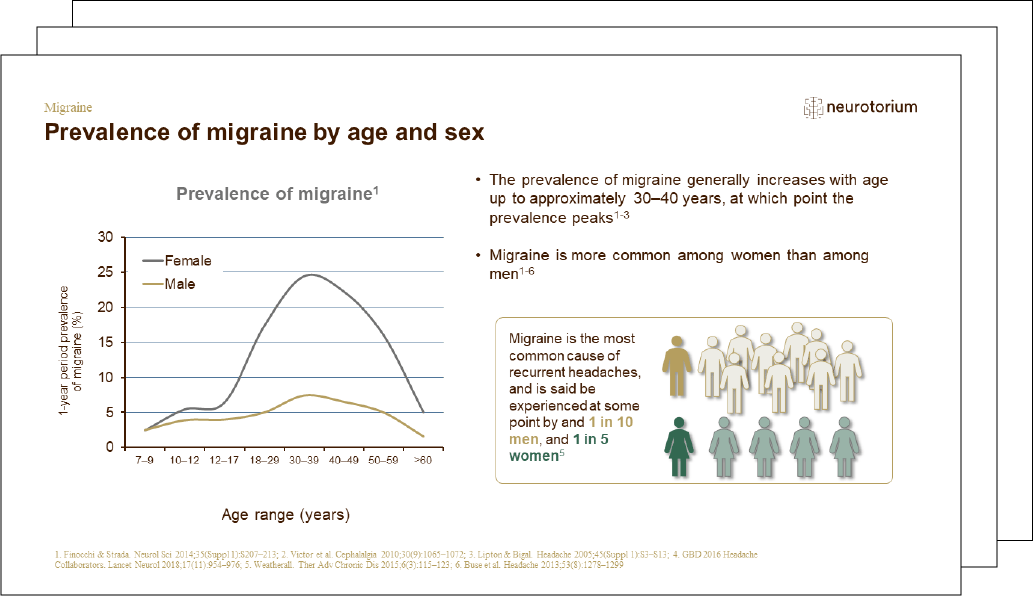
Over 1 billion people worldwide live with migraine, making it one of the most prevalent neurological disorders. Headache disorders rank second only to dental conditions in global disease burden, measured by years lived with disability. Women are about three times more likely than men to experience migraine, largely due to hormonal influences. Migraine often starts in the teens or early adulthood and may improve later in life – but for many, it is a lifelong condition.
References
Migraine attacks often include several components, although not everyone experiences all of them. Some people notice early warning symptoms, known as the prodrome, before the headache begins. This can occur hours, or even up to a day, in advance and may include neck stiffness, yawning, changes in mood, or food cravings. However, up to around 70% of individuals do not clearly recognize or report these symptoms.
In some individuals, the headache is preceded by aura, which typically lasts between 5 and 60 minutes. Visual symptoms are most common and may appear as wavy or zigzag lines, flashes of light, shimmering spots, or blind areas that gradually spread across the field of vision. Sensory symptoms, such as tingling starting in the fingers or around the mouth and spreading to the arm or face, can also occur. These symptoms usually develop gradually and may follow one another.
The headache itself is often described as throbbing or pulsating and may be felt on one side of the head, although it can also be bilateral. It can range from moderate to severe and is often aggravated by physical activity. Sensitivity to light and sound is common, sometimes also to smells, and nausea or vomiting may occur. After the headache resolves, some people experience a period of recovery known as the postdrome, which can last up to 48 hours. During this time, they may feel tired, mentally slowed, or have lingering discomfort in the neck and shoulders. Not everyone experiences all of these components. Some people have only headache and associated sensitivity, while others experience several of these features.
References
- Neurotorium. Migraine – Course, Natural History, and Prognosis. https://neurotorium.org/slidedeck/migraine-course-natural-history-and-prognosis/
- Eigenbrodt, A. K. et al. Diagnosis and management of migraine in ten steps. Nat.Rev. Neurol. 17, 501–514 (2021).
- Ashina, M. Migraine. N. Engl. J. Med. 383, 1866–1876 (2020).
Migraine is diagnosed clinically, meaning that the diagnosis is based on a person’s medical history and reported symptoms rather than on laboratory tests or brain scans. To support the diagnosis, clinicians use criteria from the International Classification of Headache Disorders (ICHD-3).
These criteria consider several key features. First, the number of attacks is assessed, and at least five attacks are usually required. Second, the duration of the headache is evaluated, which in adults typically lasts between 4 and 72 hours. Third, the characteristics of the pain are considered. Migraine pain is often described as pulsating and may be unilateral, but it can also be bilateral and does not always have a throbbing quality. The intensity is typically moderate to severe and may worsen with physical activity.
In addition, associated symptoms are important for the diagnosis. These include nausea and/or vomiting, as well as sensitivity to light and sound. The presence or absence of aura is also taken into account.
If there are any atypical features or abnormal findings on examination, further evaluation may be needed to exclude other causes, such as sinus disease, tensiontype headache, or more serious conditions.
References
- Neurotorium. Migraine – History, Definitions, and Diagnosis. https://neurotorium.org/slidedeck/migraine-history-definitions-and-diagnosis/
- Eigenbrodt, A. K. et al. Diagnosis and management of migraine in ten steps. Nat.Rev. Neurol. 17, 501–514 (2021).
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 38, 1–211 (2018).
Treatment strategies for migraine are generally divided into acute treatments and preventive treatments.
Acute treatments are taken during a migraine attack to relieve pain and associated symptoms. Simple analgesics, such as ibuprofen, aspirin, or acetaminophen, are commonly used and are most effective when taken early in the attack. Combination pills may also be helpful. Triptans are migrainespecific medications that act on serotonin receptors and reduce pain by modulating trigeminovascular signaling.
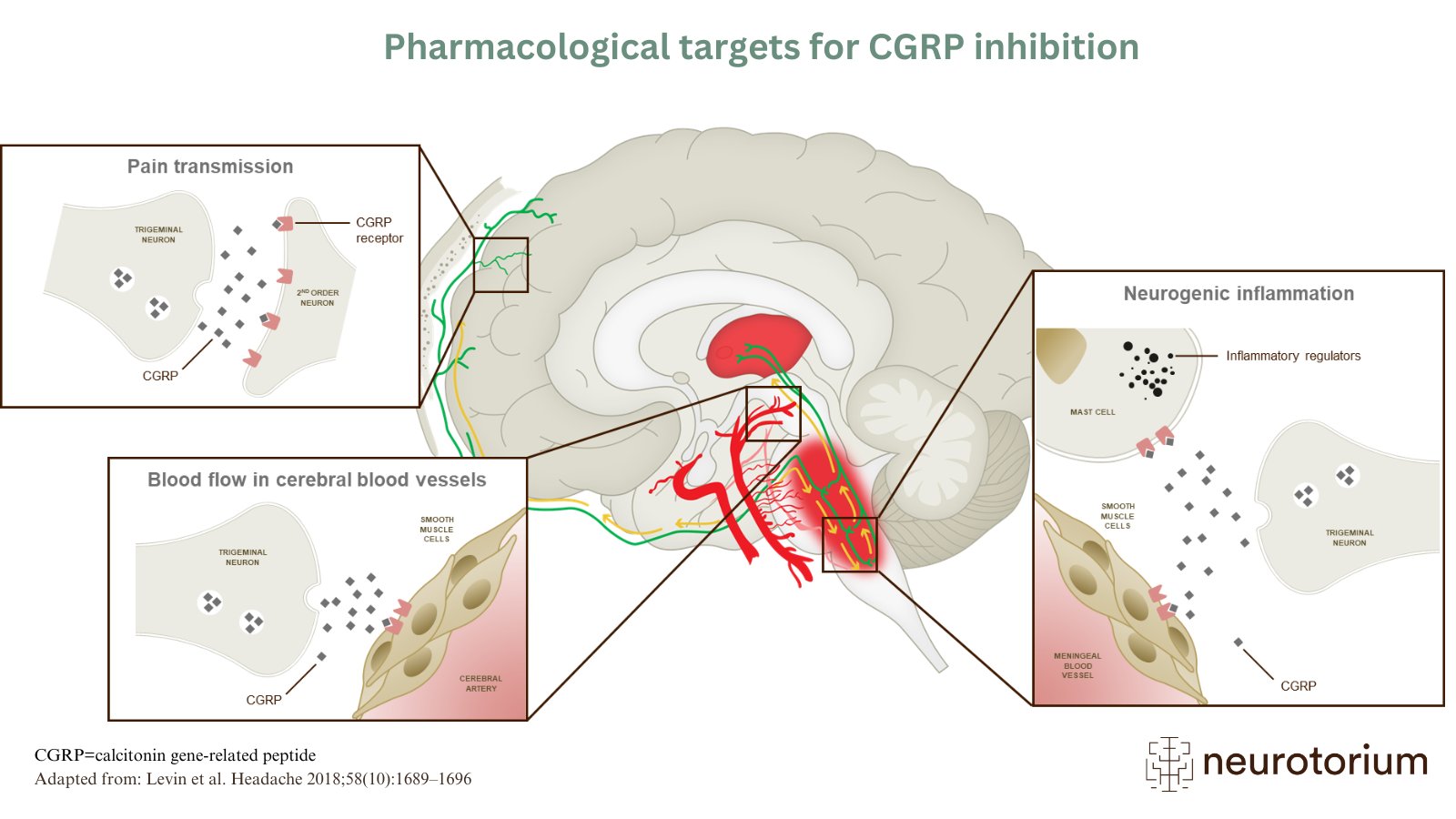
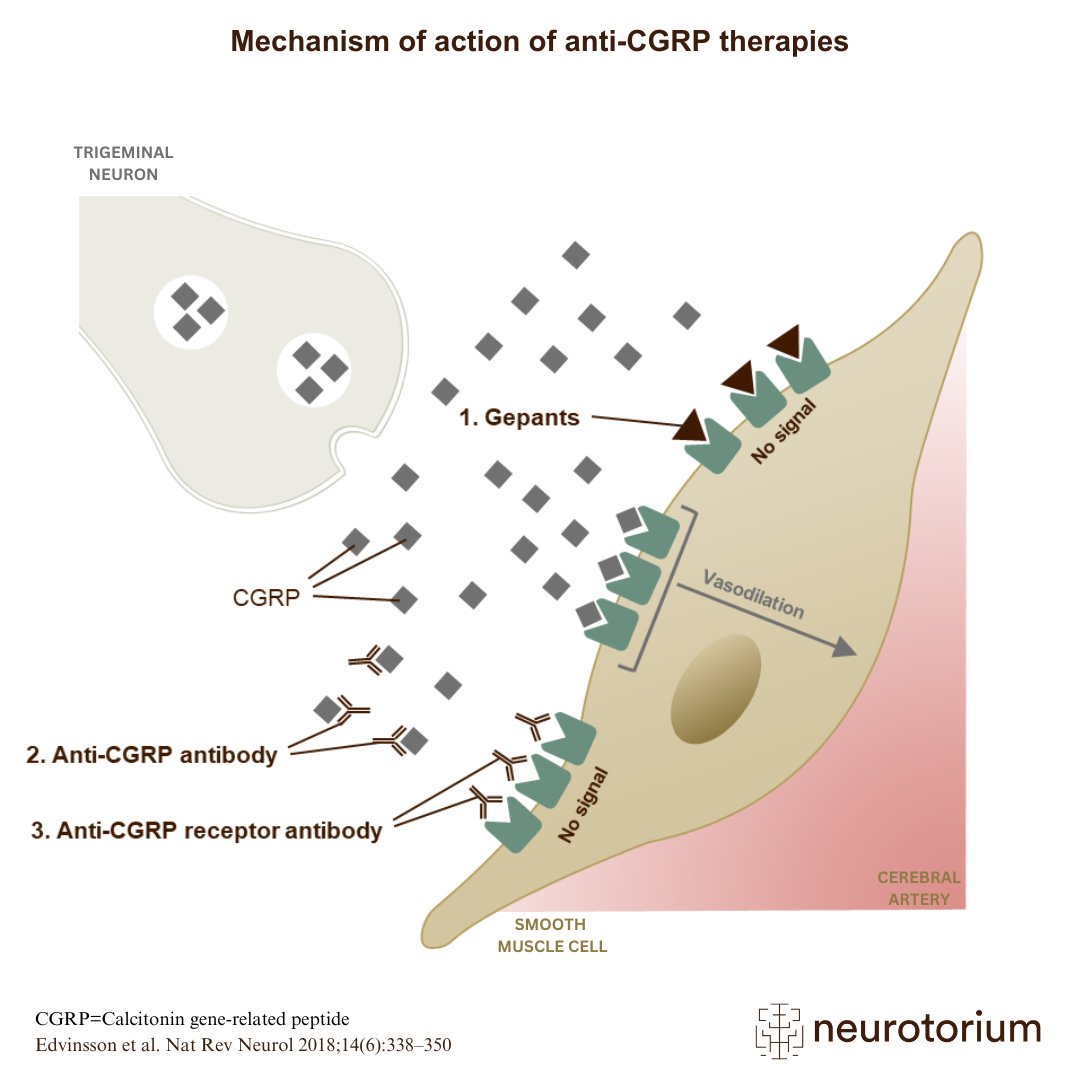
More recently, treatments targeting the calcitonin gene-related peptide (CGRP) pathway have been introduced. These include gepants, which block the CGRP receptor and can be used both for acute treatment of migraine attacks and, in some cases, as preventive therapy. Gepants are particularly useful for individuals who cannot tolerate triptans or have cardiovascular risk factors.
Preventive treatments are recommended for people with frequent or disabling migraine, typically four or more days per month. Traditional options include certain antihypertensive drugs, such as betablockers, as well as antiepileptic drugs, such as topiramate or valproate. However, antiepileptic drugs should be avoided in women of childbearing age because of the risk of birth defects and developmental complications.
In addition, monoclonal antibodies targeting the CGRP pathway, either the peptide itself or its receptor, have become an important option for migraine prevention. These treatments are generally well tolerated and can be effective in individuals who do not respond to, or cannot tolerate, conventional preventive medications. They are administered as injections, typically on a monthly or quarterly basis. When selecting treatment, both for acute and preventive use, it is important to consider expected benefit, potential side effects, and the individual patient’s clinical profile.
References
To support management and improve quality of life with migraine, it is helpful to keep a migraine diary to record attacks, noting food, sleep, stress, weather, and treatments. In addition, spotting and avoiding triggers when possible, can reduce the frequency of attacks. Maintaining healthy routines, including regular sleep, regular meals, good hydration, and gentle exercise, is also important. Furthermore, following the treatment plan by strictly taking acute medication early and preventative medication as prescribed can improve outcomes. Building a strong care team is beneficial, and referral to a headache specialist can be arranged through a general practitioner if standard management is not sufficient. Finally, exploring support groups or counselling can be valuable, as living with chronic pain can be difficult and sharing strategies can help.
References
- Antiepileptic drugs: Medications originally developed to treat epilepsy, but also effective in preventing migraines. Examples include topiramate and valproate.
- Aura: A subjective sensation that occurs before or during a migraine attack. It can include visual disturbances (such as flashing lights or zigzag lines), strange tastes or odors, numbness, or feelings of unreality or déjà vu.
- Calcitonin Gene-related Peptide (CGRP): A neuropeptide involved in various physiological processes, particularly in pain transmission and migraine pathophysiology.
- Ditans: A newer class of migraine-specific drugs that act on serotonin receptors, designed for people who cannot take triptans.
- Gepants: A newer class of medications that block CGRP, a key molecule involved in migraine pathways.
- International Classification of Headache Disorders (ICHD-3): An official system developed by the International Headache Society that provides diagnostic criteria for all headache disorders, including migraines.
- Monoclonal antibodies: Lab-engineered proteins that target specific molecules in the body. In migraine treatment, certain monoclonal antibodies block CGRP or its receptor to reduce the frequency of attacks.
- Osmophobia: An increased sensitivity to smells, often unpleasant, which can occur during a migraine attack.
- Phonophobia: Sensitivity to sound, commonly experienced during migraine attacks.
- Photophobia: Sensitivity to light, one of the most frequent symptoms associated with migraine.
- Simple analgesics: Common over-the-counter pain relievers such as ibuprofen, aspirin, and acetaminophen, which may help relieve mild to moderate migraine attacks.
- Trigger factors: Specific stimuli or conditions that can provoke a migraine attack. These include stress, hormonal changes, certain foods, environmental factors, and lack of sleep.
- Triptans: A class of migraine-specific medications (such as sumatriptan) that act on serotonin receptors and can effectively stop an attack if taken early.
References
- Eigenbrodt, A. K. et al. Diagnosis and management of migraine in ten steps. Nat.Rev. Neurol. 17, 501–514 (2021).
- Ashina, M. Migraine. N. Engl. J. Med. 383, 1866–1876 (2020).
- Migraine Glossary – Migraine Research Foundation. Home – Migraine Research Foundation https://migraineresearchfoundation.org/about-migraine/migraineglossary/.
- Glossary. American Migraine Foundation. https://americanmigrainefoundation.org/glossary/.
- Delussi, M., Laporta, A., Fraccalvieri, I. & de Tommaso, M. Osmophobia in primary headache patients: associated symptoms and response to preventive treatments. J. Headache Pain 22, 109 (2021).
- Cleveland Clinic. Antiseizure medication. Cleveland Clinic https://my.clevelandclinic.org/health/treatments/24781-antiseizure-medicationsanticonvulsants.
3D Brain Atlas
Some areas of the brain seem to be particularly related to migraine:
- The trigeminal nerve, the fifth cranial nerve, together with the brain stem, forms the trigeminal complex. Several lines of research point to the importance of this complex for migraine.
- Thalamus appears to be important for several processes underlying migraine, such as allodynia and central sensitisation.