Slide Decks on Alzheimer’s Disease
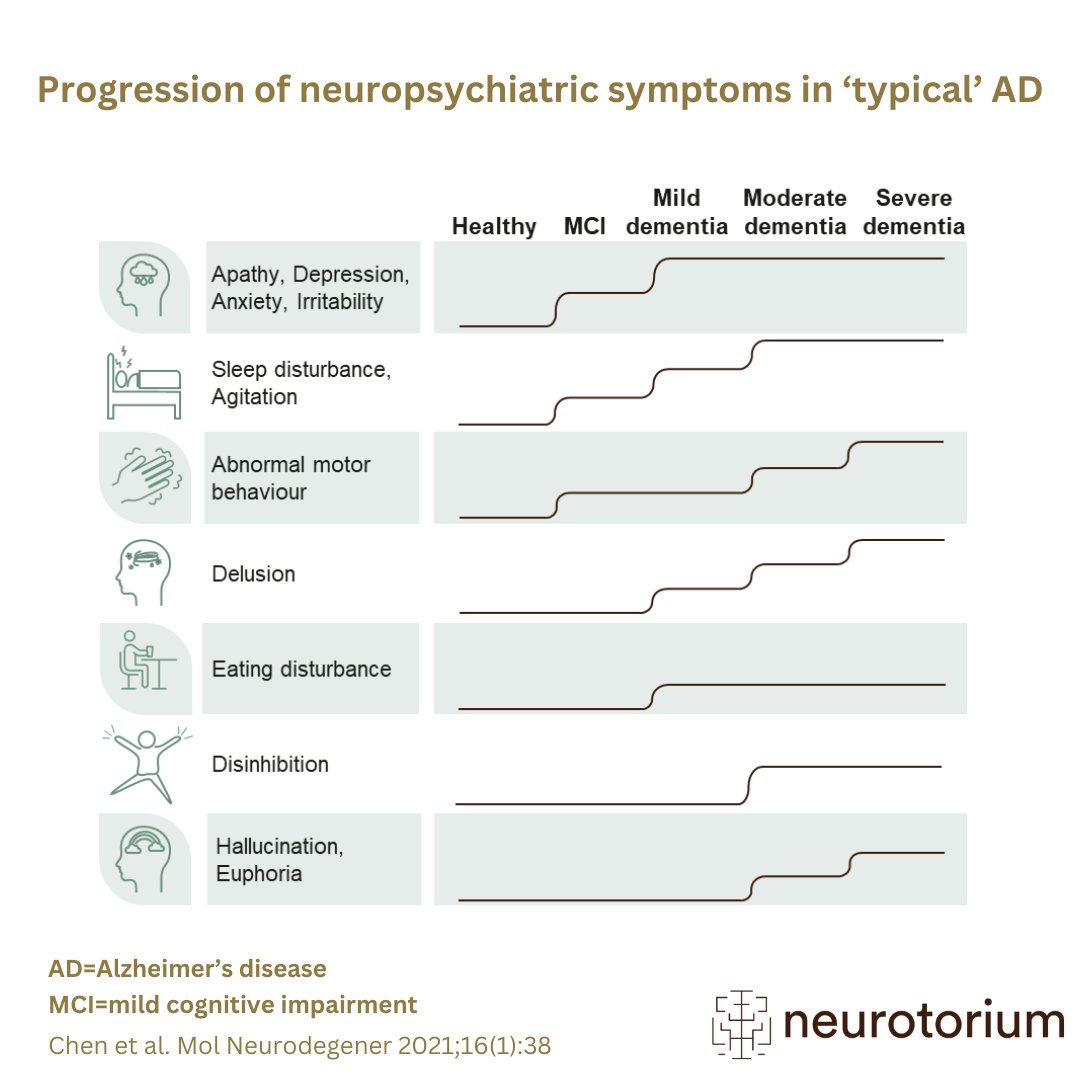
Alzheimer’s disease (AD) is a neurodegenerative disease that causes gradual cognitive decline and dementia. AD symptoms can be divided into three categories – cognitive, functional, and neuropsychiatric. Some neuropsychiatric symptoms (NPS) are key clinical manifestations of AD, with evidence that the prevalence of NPS increases with the severity of cognitive impairment. Particularly, symptoms of agitation, delusion, and irritability have been associated with worse cognitive performance.
Get an introduction to what is currently known about AD by going through our slide decks. Our slide deck is free to download and use in your presentations.
Would you like to learn more about Alzheimer’s risk factors and prevention strategies?
Definitions and Diagnosis
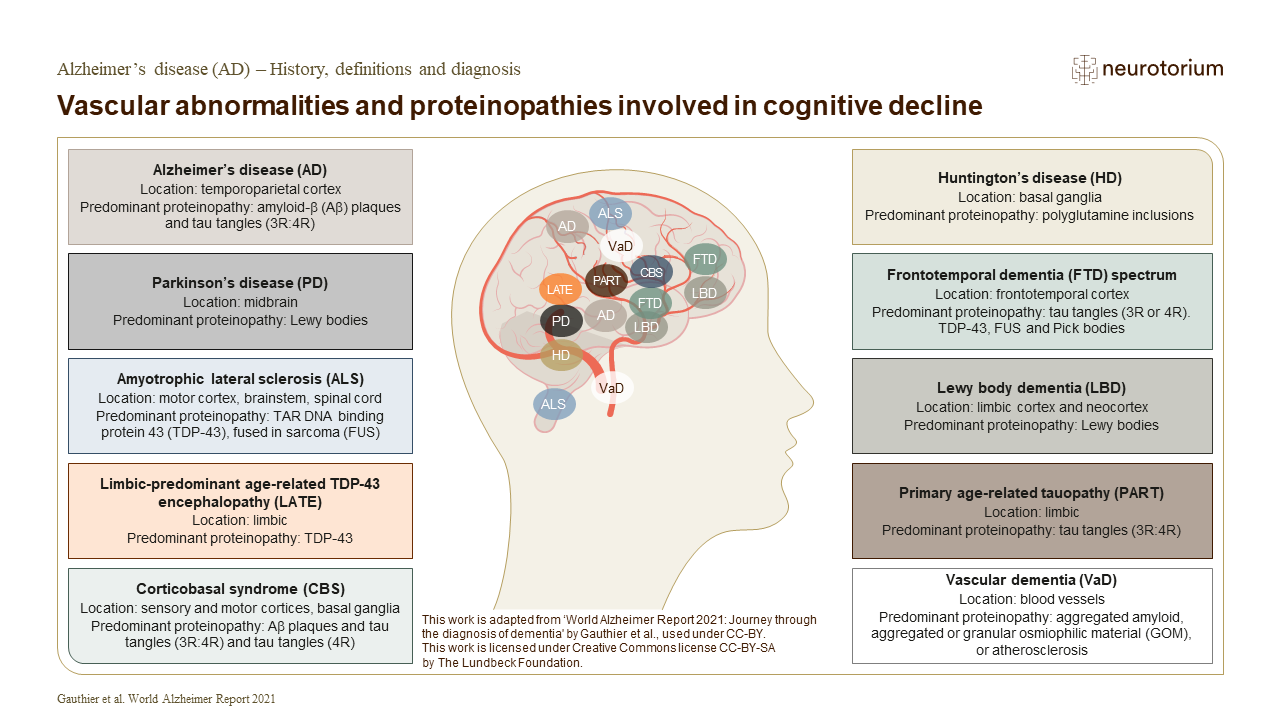
Alzheimer’s disease (AD) refers to the abnormal presence of Aβ and tau proteins, which define AD among many other neurodegenerative diseases. Go to the slide deck.
Epidemiology and Burden
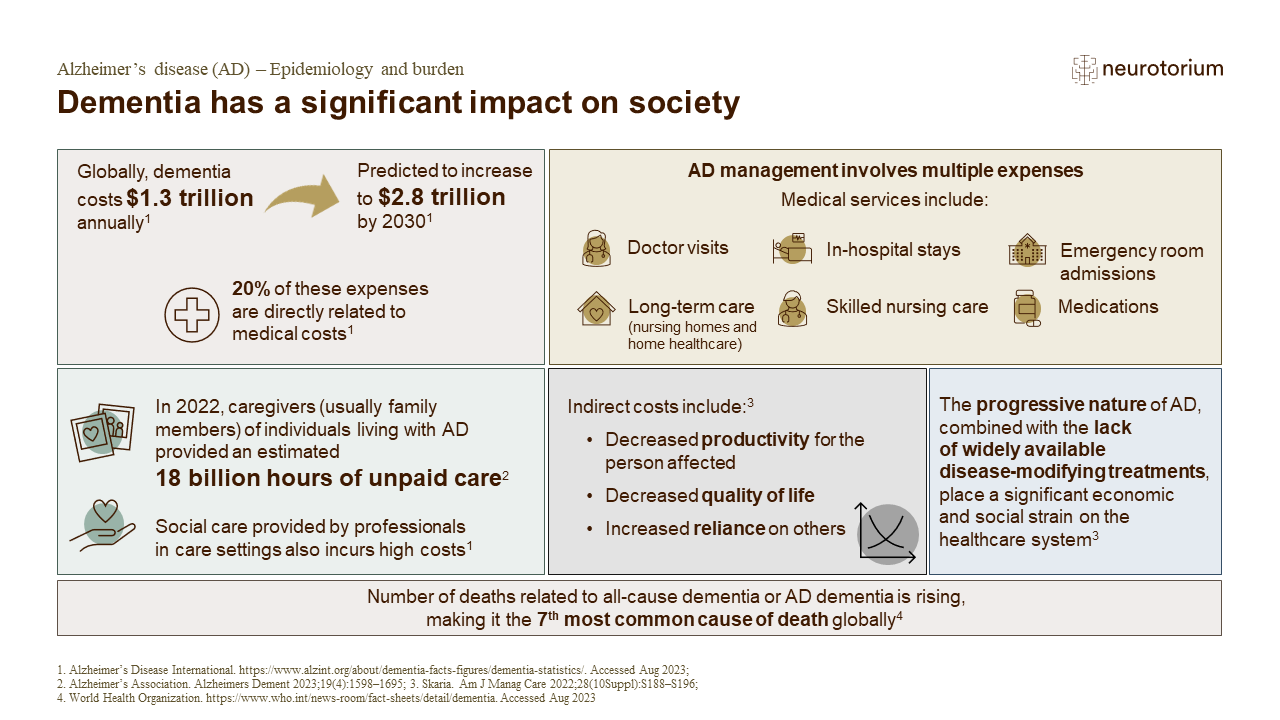
This slide deck discusses the epidemiology and burden of AD and highlights topics as prevalence of dementia, burden of AD and the assessment scales for the quality of life and resource utilization in dementia. Go to the slide deck.
Neurobiology and Aetiology
This slide deck discusses neurobiology and aetiology for AD and highlights topics as risk factors, pathopsysiological hypotheses, and the development and importance of biomarkers. Go to the slide deck.
Course, Natural History and Prognosis
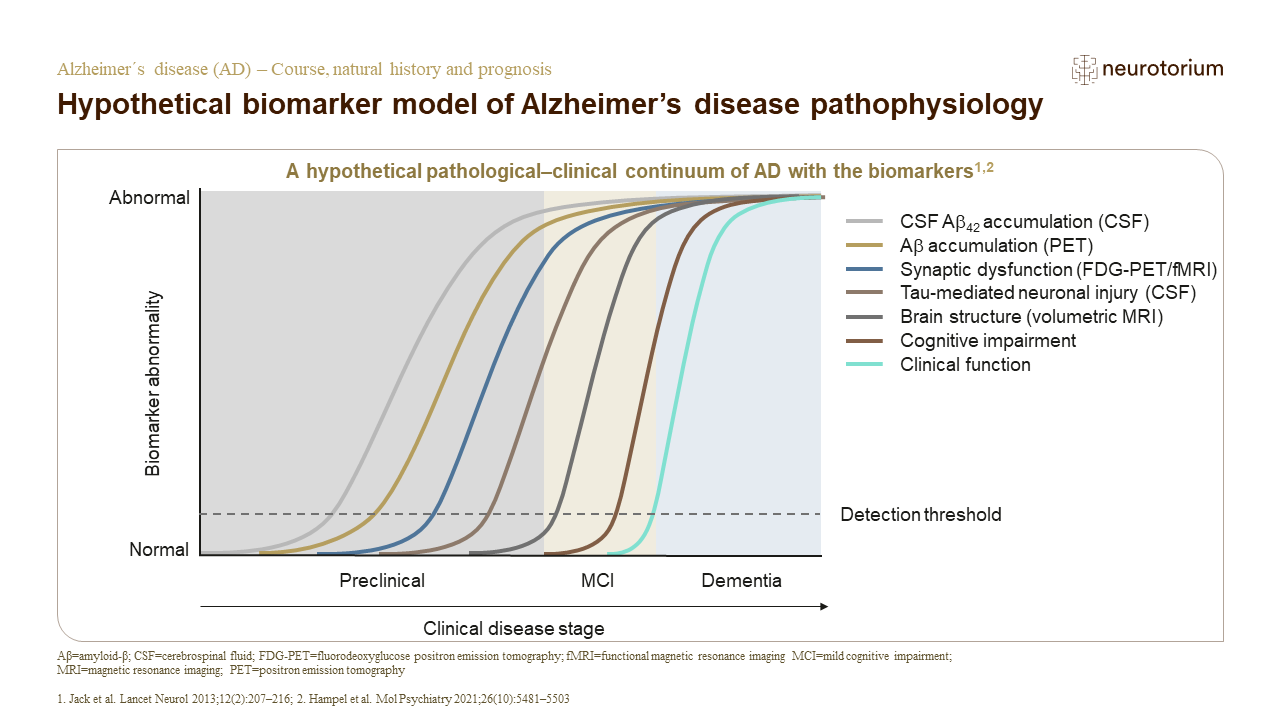
This slide deck discusses in detail the course, natural history and prognosis of AD, with illustrations. Go to the slide deck.
Comorbidities
This slide deck describes current knowledge on the general medical and psychiatric comorbidities of AD. Go to the slide deck.
Treatment Principles
In this slide deck you will find basic concepts and definitions related to approaches such as disease-stage-specific treatment and psychosocial therapies. Go to the slide deck.
Articles on Alzheimer’s Disease
Considerable advancements in AD research have been made over the years, working towards a reality of early identification with in-vivo biomarkers and multimodal treatment of patients with AD. Several disease-modifying therapies, such as agents targeting amyloid accumulation, tau pathology, and others, are being investigated.
- The Physical and Social Exposome in Brain Health and Dementia
 The exposome reframes dementia as the product of cumulative physical and social exposures-like pollution, nutrition, and inequality-across life. These factors shape brain aging through inflammation and epigenetic change. Lifespan, global studies are key to equitable dementia prevention.
The exposome reframes dementia as the product of cumulative physical and social exposures-like pollution, nutrition, and inequality-across life. These factors shape brain aging through inflammation and epigenetic change. Lifespan, global studies are key to equitable dementia prevention. - Next steps for improving clinical trial outcomes in neurodegenerative disease
 This article discusses potential next steps for enhancing clinical trial outcomes in neurodegenerative diseases, with the ultimate goal of improving patient care
This article discusses potential next steps for enhancing clinical trial outcomes in neurodegenerative diseases, with the ultimate goal of improving patient care - Global perspectives on Alzheimer’s disease diagnosis and treatment: challenges and considerations in resource-limited settings
 Alzheimer’s disease (AD) is the most prevalent neurodegenerative disease and the leading cause of dementia worldwide, regardless of socioeconomic status.
Alzheimer’s disease (AD) is the most prevalent neurodegenerative disease and the leading cause of dementia worldwide, regardless of socioeconomic status.
Watch The Videos on Alzheimer’s Disease
Access our series of videos, where we complement recent articles by explaining complex topics, breaking down detailed figures, discussing current issues, and illustrating key concepts. Dive into the varying severity of cognitive impairment in individuals living with Alzheimer’s Disease (AD) and the importance of early diagnosis for effective care, among other crucial topics.

Alzheimer’s Disease Biomarkers
In this video Joseph Therriault, PhD discusses the AD biomarkers and their use in clinical and research settings and explore future research areas for wider clinical practice use.

Alzheimer’s Disease is not synonymous with dementia
In this video, Professor Dr. Serge Gauthier explains what dementia is and what differentiates Alzheimer’s disease from other types of dementias.
The Complexities and Prospects of Dementia Care in the Future
In this video, Professor Matthew Kiernan discusses the complexities of dementia research, including recent insights into neurobiological aetiologies, and promising developments for therapeutics.
Download Illustrations & Figures on Alzheimer’s Disease
Download and utilize images illustrating pertinent aspects of Alzheimer’s disease. Selected images provide insights into high-performing CSF and plasma biomarkers summarizing Alzheimer’s disease diagnosis, brain metabolism PET imaging in Alzheimer’s disease, and Amyloid-PET imaging in Alzheimer’s disease.
Frequently Asked Questions (FAQ)
The information provided in this document is for educational purposes only and is not a substitute for medical care. If you have questions about your health, speak with a healthcare professional.
Alzheimer’s disease (AD) is the most common form of dementia, responsible for 50–75% of all cases. AD gradually affects the brain, causing issues with memory, thinking, language and behaviour. As it progresses, AD can also bring changes in mood and a reduced ability to manage day-to-day tasks.
References
- Neurotorium. Alzheimer’s Disease – Definitions and Diagnosis. https://neurotorium.org/slidedeck/alzheimers-disease-history-definitions-and-diagnosis/
- What is Dementia? Symptoms, Causes & Treatment | alz.org. Accessed January 9, 2024. https://www.alz.org/alzheimers-dementia/what-is-dementia
- ADI – Dementia facts & figures. Accessed January 9, 2024. https:// www.alzint.org/about/dementia-facts-figures/
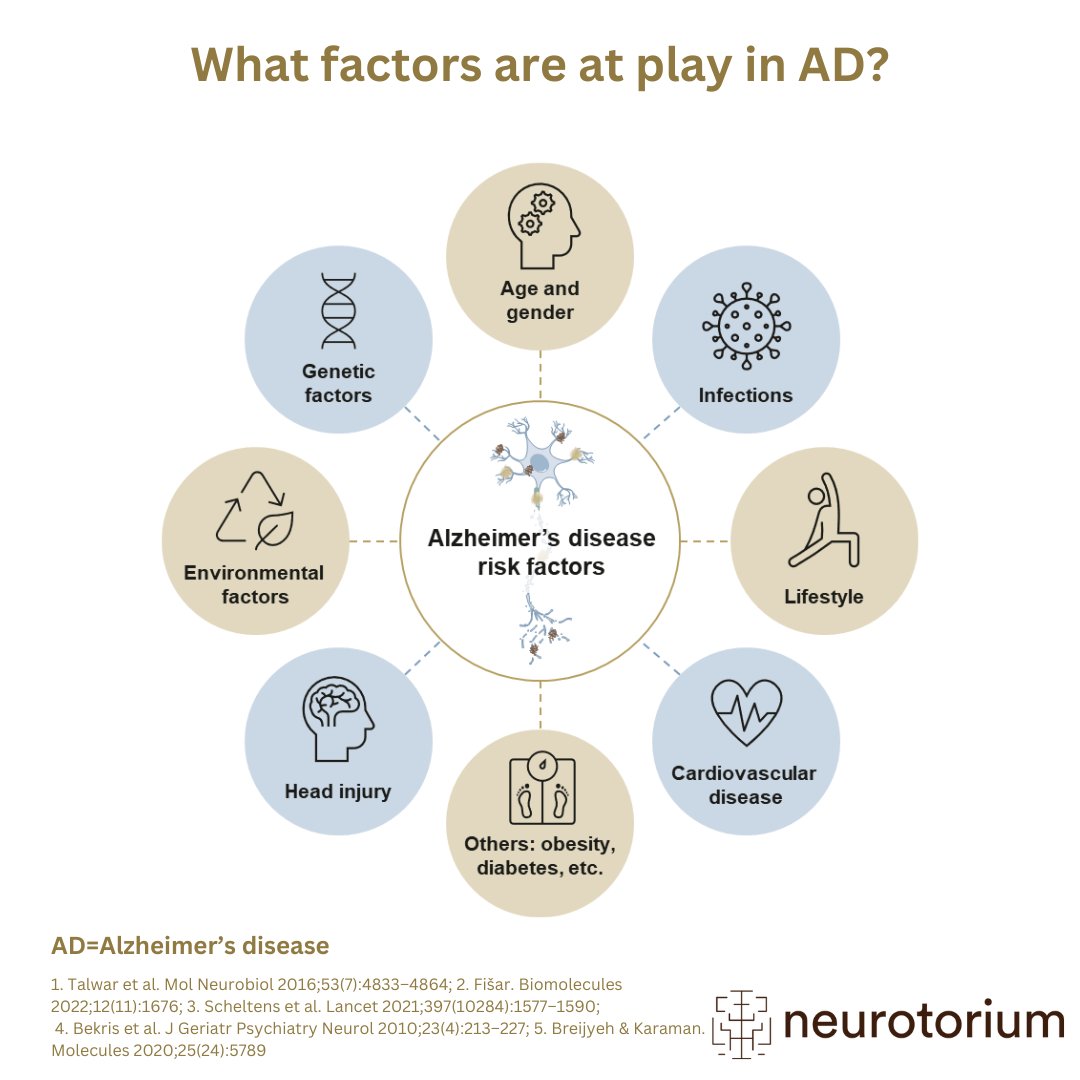
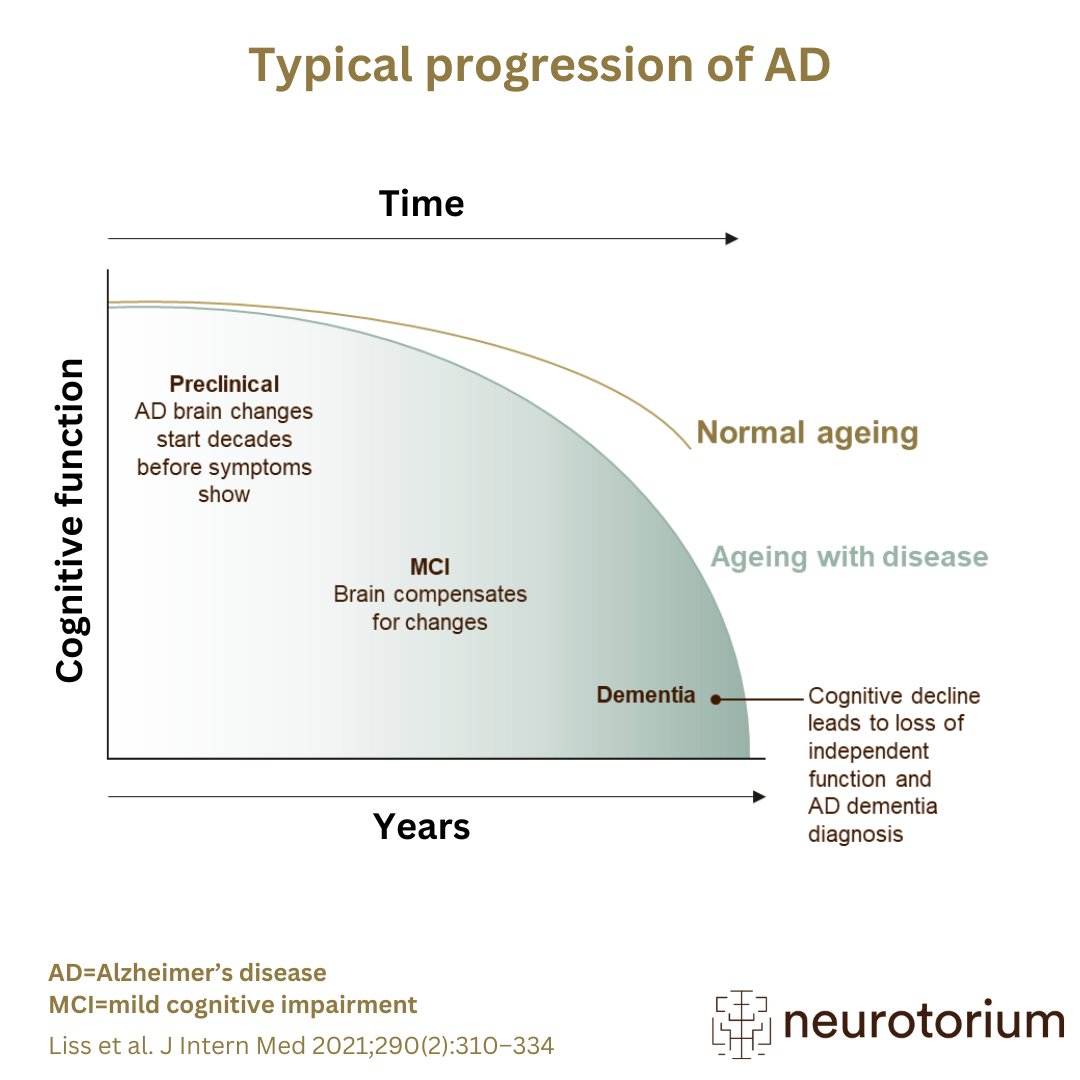
The exact cause of AD is unknown, but it’s linked to the harmful buildup of protein material in the brain (especially two proteins called amyloid and tau). The risk of developing AD is influenced by age, genetics, environment, and lifestyle factors. Age plays a major role in the development of AD; the older a person is, the higher the risk. While rare, young adults can also develop AD. About one in ten cases of AD occurs in people who are below the age of 65 years, and this is referred to as early-onset AD. The brain changes leading to AD begin many years before symptoms appear. A healthy lifestyle is linked to a lower risk of AD and other types of dementia.
References
- Neurotorium. Alzheimer’s Disease – Neurobiology and Aetiology. https://neurotorium.org/slidedeck/neurobiology-and-aetiology/
- ADI – Dementia facts & figures. Accessed January 9, 2024. https:// www.alzint.org/about/dementia-facts-figures/
- Dementia, Your Companion Guide. Dementia Education Program. June 2023. Accessed January 9, 2024. https://www.mcgill.ca/dementia/ resources/dementia-your-companion-guide
AD, along with other forms of dementia, is becoming more common worldwide. As of 2021, about 57 million people were living with dementia worldwide. The total number of people living with dementia is expected to reach 139 million by 2050, with the largest increase occurring in low- and middle-income countries. The actual figures might be even higher because some cases are not diagnosed correctly or are overlooked altogether. This means more people are likely affected by AD than current estimates suggest.
References
- Neurotorium. Alzheimer’s Disease – Epidemiology and Burden. https://neurotorium.org/slidedeck/alzheimers-disease-epidemiology-and-burden/
- ADI – Dementia statistics. Accessed January 9, 2024. https://www. alzint.org/about/dementia-facts-figures/dementia-statistics/
- Tahami Monfared AA, Byrnes MJ, White LA, Zhang Q. Alzheimer’s Disease: Epidemiology and Clinical Progression. Neurol Ther. 2022;11(2):553-569. doi:10.1007/s40120-022-00338-8
- WHO. Dementia. World Health Organization. Accessed January 28, 2026. https://www.who.int/news-room/fact-sheets/detail/dementia
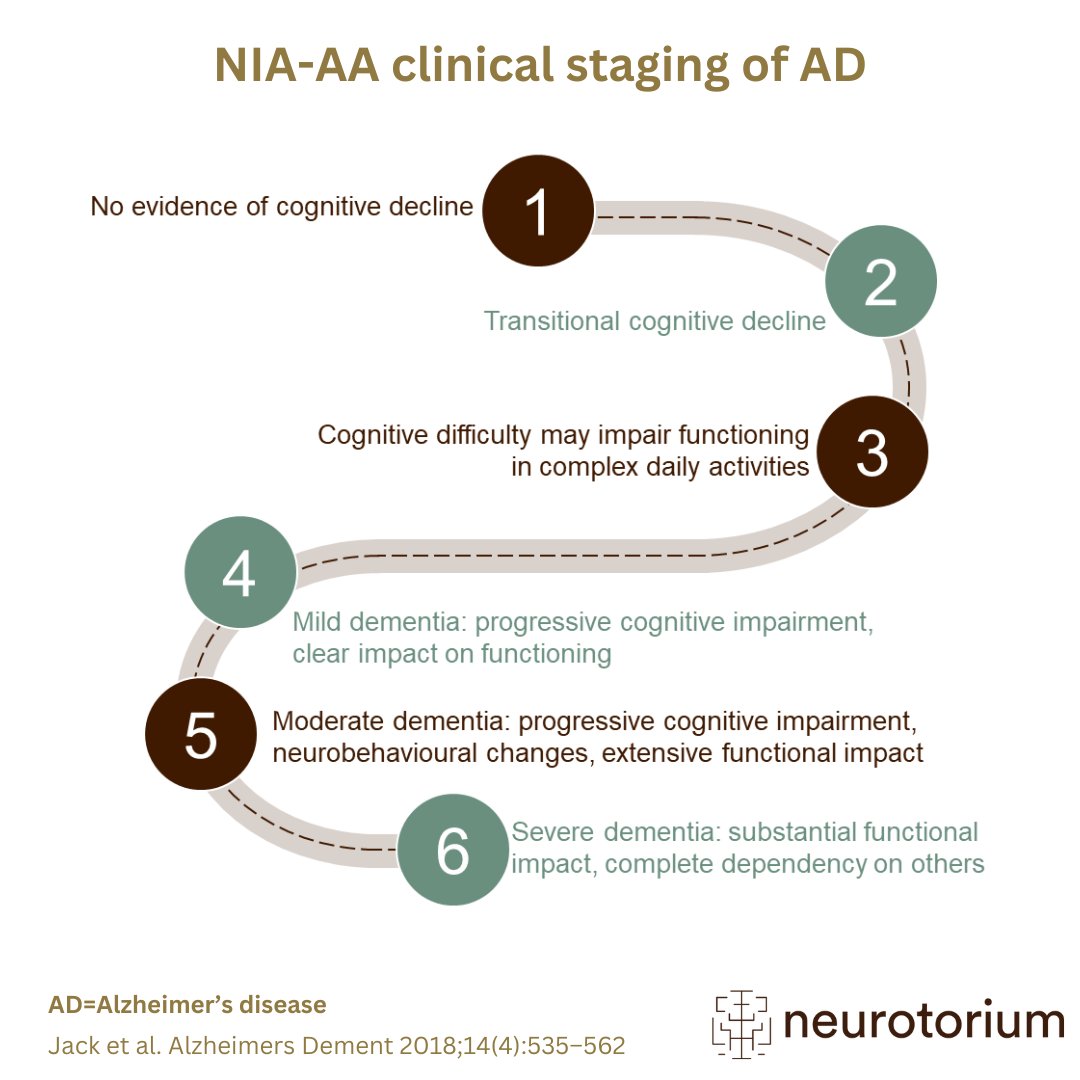
AD symptoms fall into three main categories: cognitive, functional, and neuropsychiatric symptoms. The symptoms of AD tend to worsen gradually over time, but how quickly this happens varies from person to person. The main area of cognition that is impaired during AD is memory, with additional changes to language, attention, executive functions, and visuospatial function. AD usually begins with forgetfulness in everyday matters, such as getting lost, losing everyday items, repetitive conversations, or forgetting names. It can also affect the ability to understand and use words. Concentrating and decision-making become challenging, and there may be difficulties recognizing familiar things or navigating both familiar and unfamiliar places. As AD progresses, everyday tasks become harder to carry out. These are referred to as the functional symptoms of AD. Daily tasks like driving, cooking, dressing, and managing finances become increasingly difficult, with an impact on the person with AD and a significant burden on caregivers. Neuropsychiatric symptoms (NPS), refer to mental and emotional aspects, such as apathy, depression or agitation. Most people with AD have NPS at some point in their illness. These symptoms are associated with a lower quality of life, an earlier need for advanced care, a faster decline in thinking abilities, and increased stress for caregivers.
References
- Neurotorium. Alzheimer’s Disease – Course, Natural History and Prognosis. https://neurotorium.org/slidedeck/alzheimers-disease-ad-course-natural-history-and-prognosis/
- Joubert S, Joncas S, Barbeau E, Joanette Y, Ska B. Cognition. In: Clinical Diagnosis and Management of Alzheimer’s Disease. Third. 2007:12. https://doi.org/10.3109/9780203931714
- Gélinas I. Functional autonomy. In: Clinical Diagnosis and Management of Alzheimer’s Disease. Third. 2007:12. https://doi.org/ 10.3109/9780203931714
- Steinberg M, Shao H, Zandi P, et al. Point and 5-year period prevalence of neuropsychiatric symptoms in dementia: the Cache County Study. Int J Geriatr Psychiatry. 2008;23(2):170-177. doi:10.1002/ gps.1858
- Burke AD, Goldfarb D, Bollam P, Khokher S. Diagnosing and Treating Depression in Patients with Alzheimer’s Disease. Neurol Ther. 2019;8(2):325-350. doi:10.1007/s40120-019-00148-5
Although the diagnostic journey for an individual with AD differs around the world, in many countries, the first step involves a visit to the primary care doctor. They may then refer the person with symptoms to a memory assessment service. These specialist services may be led by a neurologist, psychiatrist, geriatrician, or specialist nurse. For diagnosis, they will typically ask about the signs and symptoms of concern from the individual with cognitive symptoms, or from their family / friends. In the process of determining whether someone has AD, the doctor may:
1. Ask about the person’s medical history and talk to someone close for additional information.
2. Check how well the memory, daily activities, behaviour, and mental state are working, usually with some standardized memory tests.
3. Perform a physical check-up and run blood tests to rule out other health issues that might affect cognitive function. The physician will also review medications to see if they could be affecting cognition.
4. Use certain tests, like brain scans, specialist blood tests, or spinal fluid checks, to look for signs of AD and rule out other causes.
References
- Neurotorium. Alzheimer’s Disease – Definitions and Diagnosis. https://neurotorium.org/slidedeck/alzheimers-disease-history-definitions-and-diagnosis/
- International AD, University M. World Alzheimer Report 2021: Journey through the diagnosis of dementia. Published online September 21, 2021. Accessed January 9, 2024. https://www.alzint.org/resource/ world-alzheimer-report-2021/
Managing AD involves coordination between the doctor, the person living with AD, caregivers, and other health and social care professionals. It’s a stepby- step process that needs a group effort. Because AD gets worse over time, the person’s treatment plan must be kept up to date to address new issues. Doctors may prescribe medications, and non-drug interventions, such as psychosocial interventions, based on the individual’s needs. Symptomatic treatments are widely available in many countries. New disease-modifying therapies are becoming available in certain parts of the world. Symptomatic treatments aim to reduce the neuropsychiatric, functional, and cognitive symptoms. New disease-modifying therapies may help slow down the progression of the disease itself.
Current disease-modifying treatments are not suitable for everyone. Psychosocial interventions for AD symptoms include stimulation, behavioural, and emotion-oriented therapies. Stimulation therapies involve activities such as crafts and games, while behavioural-oriented treatments target behavioural and psychological symptoms, such as agitation, aggression, sleep disturbance, care refusal, anxiety/depression, apathy, etc. Emotion-oriented therapies, like reminiscence therapy, aim to improve mood. Appropriate psychosocial therapies for person living with AD should be selected based on the availability and the person’s preferences.
References
- Neurotorium. Alzheimer’s Disease – Treatment Principles. https://neurotorium.org/slidedeck/alzheimers-disease-treatment-principles-2/
- Atri A. The Alzheimer’s Disease Clinical Spectrum: Diagnosis and Management. Med Clin North Am. 2019;103(2):263-293. doi:10.1016/j. mcna.2018.10.009
- Rabins PV, Rovner BW, Rummans T, Schneider LS, Tariot PN. Guideline Watch (October 2014): Practice Guideline for the Treatment of Patients With Alzheimer’s Disease and Other Dementias. Focus Am Psychiatr Publ. 2017;15(1):110-128. doi:10.1176/appi.focus.15106
- APA Work Group on Alzheimer’s Disease and other Dementias, Rabins PV, Blacker D, et al. American Psychiatric Association practice guideline for the treatment of patients with Alzheimer’s disease and other dementias. Second edition. Am J Psychiatry. 2007;164(12 Suppl):5-56.
- World Alzheimer Report 2022: Life after diagnosis: Navigating treatment, care and support. Published online September 21, 2022. Accessed January 10, 2024. https://www.alzint.org/resource/world- alzheimer-report-2022/
- Scales K, Zimmerman S, Miller SJ. Evidence-Based Nonpharmacological Practices to Address Behavioral and Psychological Symptoms of Dementia. The Gerontologist. 2018;58(suppl_1):S88-S102. doi:10.1093/geront/gnx167
Family and caregiver support is a key part of the management for those living with AD. As the disease advances, individuals with AD become increasingly dependent on caregivers. Consequently, the pressure on caregivers increases. Following research on the needs of caregivers, there have been studies on support programs. Psychoeducational training for caregivers of people living with dementia has been shown to improve the quality of life of the carers.
References
- Neurotorium. Alzheimer’s Disease – Epidemiology and Burden. https://neurotorium.org/slidedeck/alzheimers-disease-epidemiology-and-burden/
- APA Work Group on Alzheimer’s Disease and other Dementias, Rabins PV, Blacker D, et al. American Psychiatric Association practice guideline for the treatment of patients with Alzheimer’s disease and other dementias. Second edition. Am J Psychiatry. 2007;164(12 Suppl):5-56.
- World Alzheimer Report 2022: Life after diagnosis: Navigating treatment, care and support. Published online September 21, 2022. Accessed January 10, 2024. https://www.alzint.org/resource/world- alzheimer-report-2022/
- Apathy is the absence of motivation, goal-oriented behaviour, and care for oneself and one’s environment.
- Cognitive function refers to mental processes such as learning, memory, ent.
- Executive functions are higher-level cognitive processes such as planning, decision-making, and working memory. Deficits in executive functioning, observed in disorders like AD, can impact the ability to manage distractions.
- Visuospatial function refers to perceiving what and where things are in the world around one.
References
- ADI – Dementia facts & figures. Accessed January 9, 2024. https:// www.alzint.org/about/dementia-facts-figures/
- APA Dictionary of Psychology. Accessed January 9, 2024. https://dictionary.apa.org/
- Sano M, Cummings J, Auer S, et al. Agitation in cognitive disorders: Progress in the International Psychogeriatric Association consensus clinical and research definition. Int Psychogeriatr. Published online March 7, 2023:1-13. doi:10.1017/S1041610222001041
3D Brain Atlas
Studies indicate that biological changes in the brain begin approximately two decades before the clinical onset of AD symptoms[1]
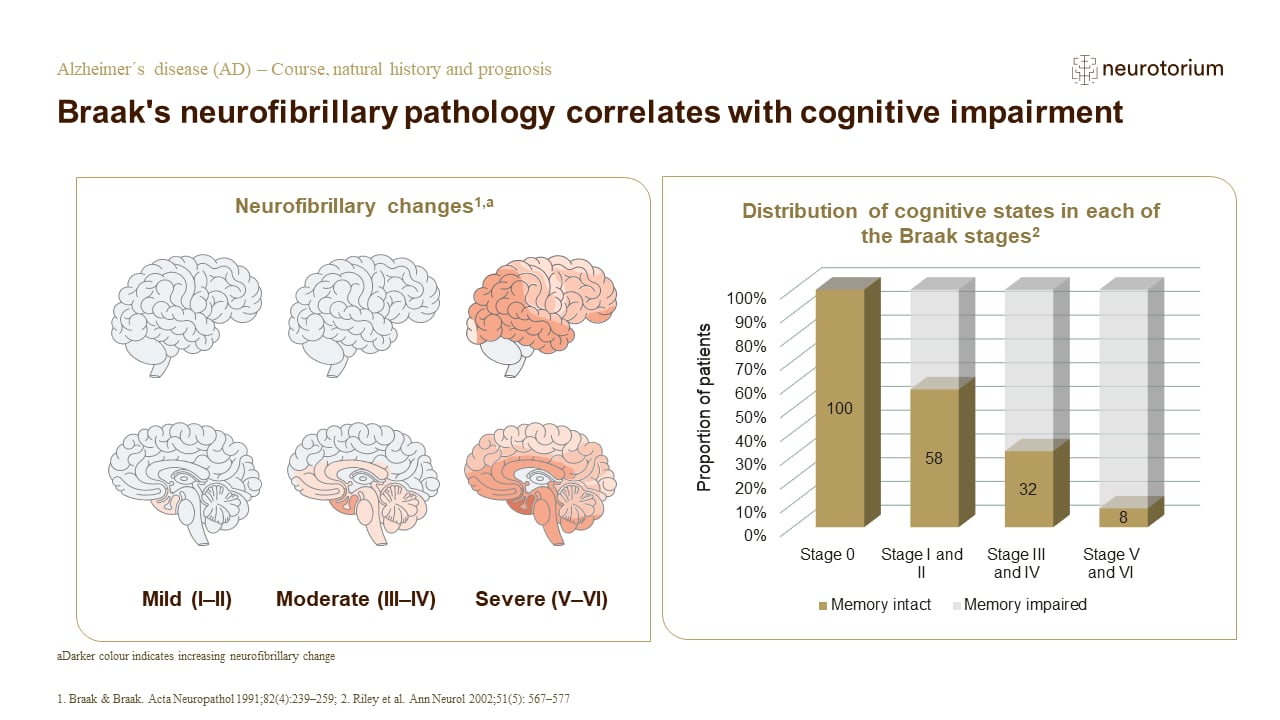
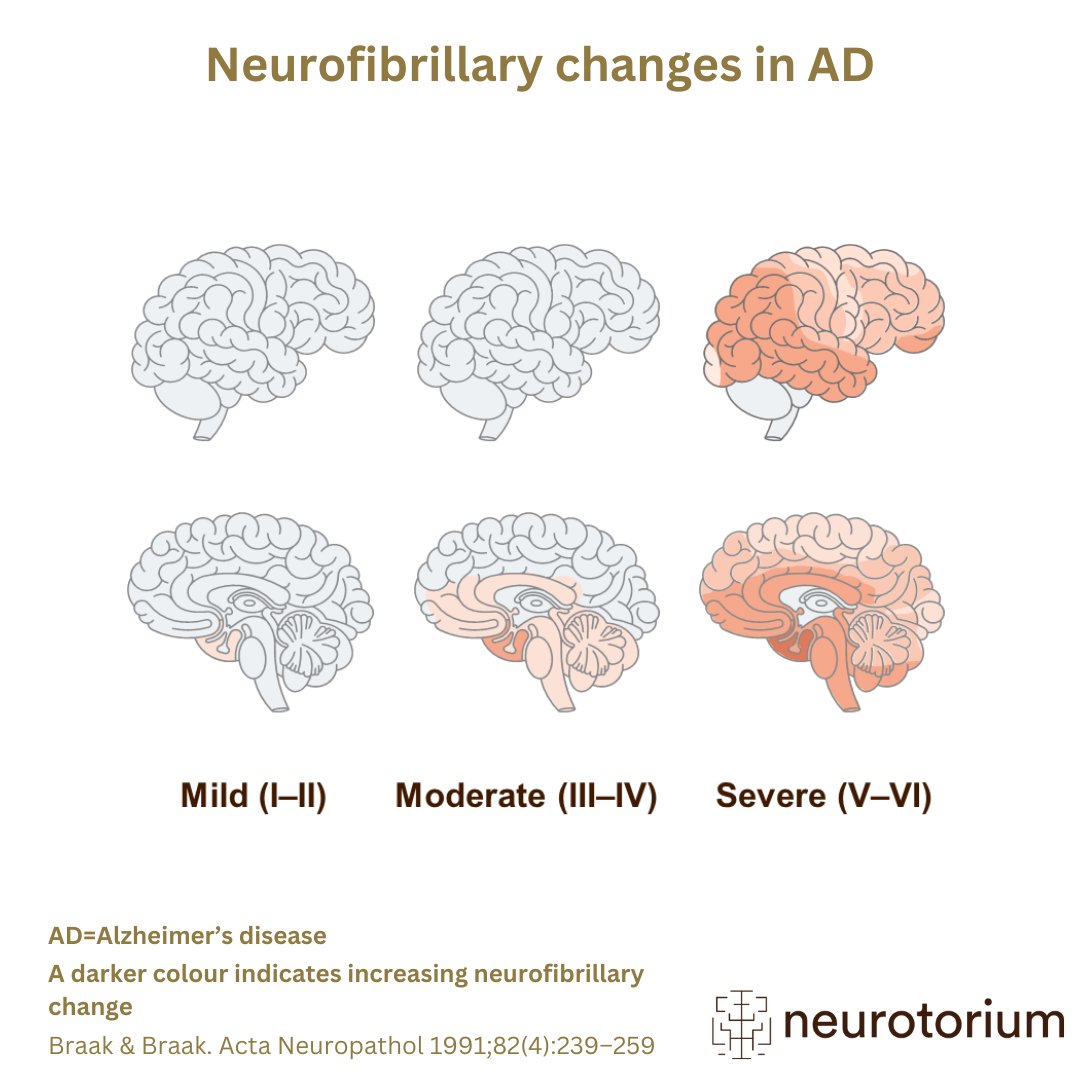
- The staging method developed by Braak and Braak suggests that the neurofibrillary pathology of AD progresses in a relatively predictable sequence across the medial temporal lobe structures, subcortical nuclei, and neocortical areas of the brain in seven stages, with the final stage representing the presence of cortical neurofibrillary changes.
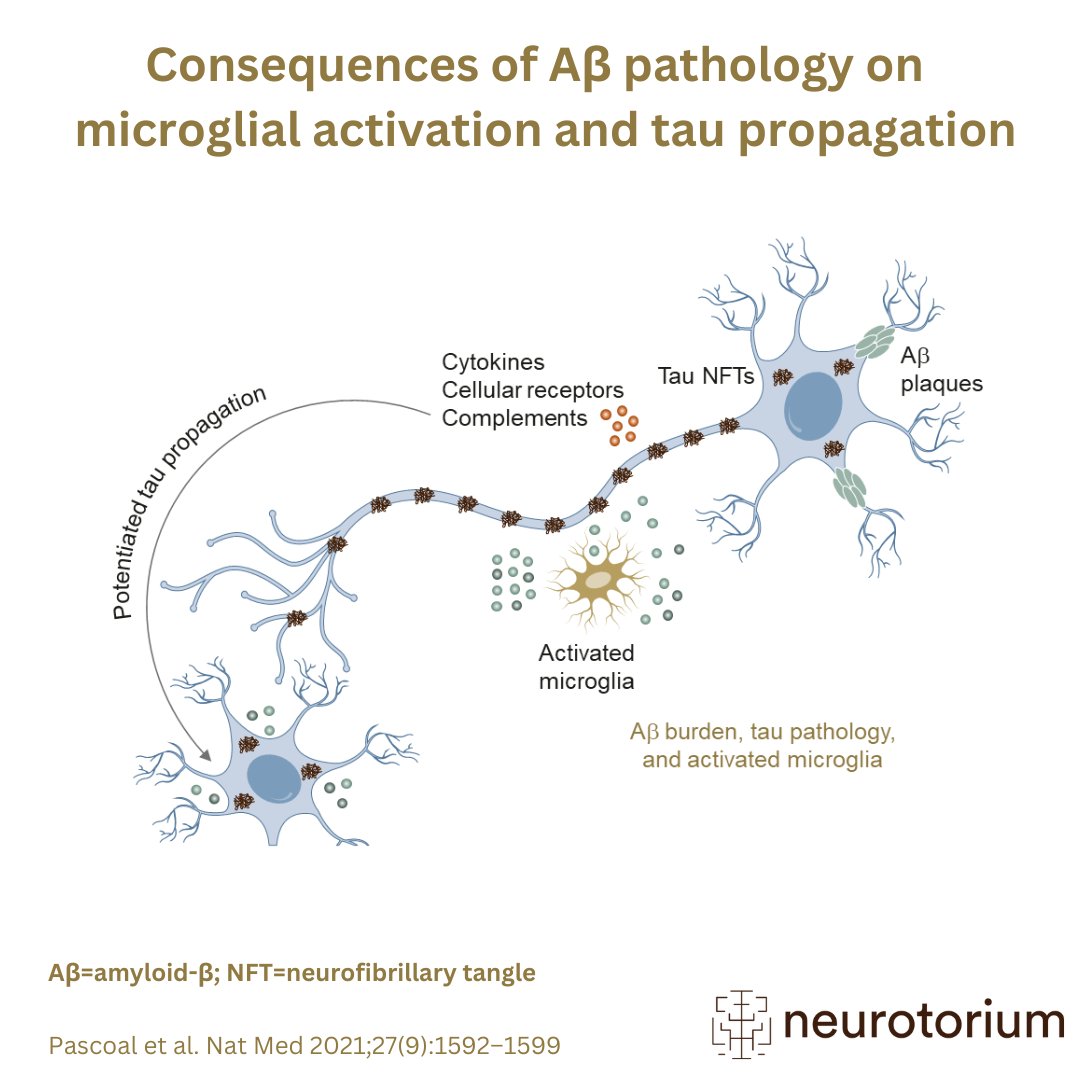
- In vivo neuroimaging data from neuropathological studies show a spatiotemporal development of Aß deposits in the brain, which originates in the cerebral regions and spreads from the neocortex, to the allocortex, to the brainstem, finally reaching the cerebellum.[2,3]