

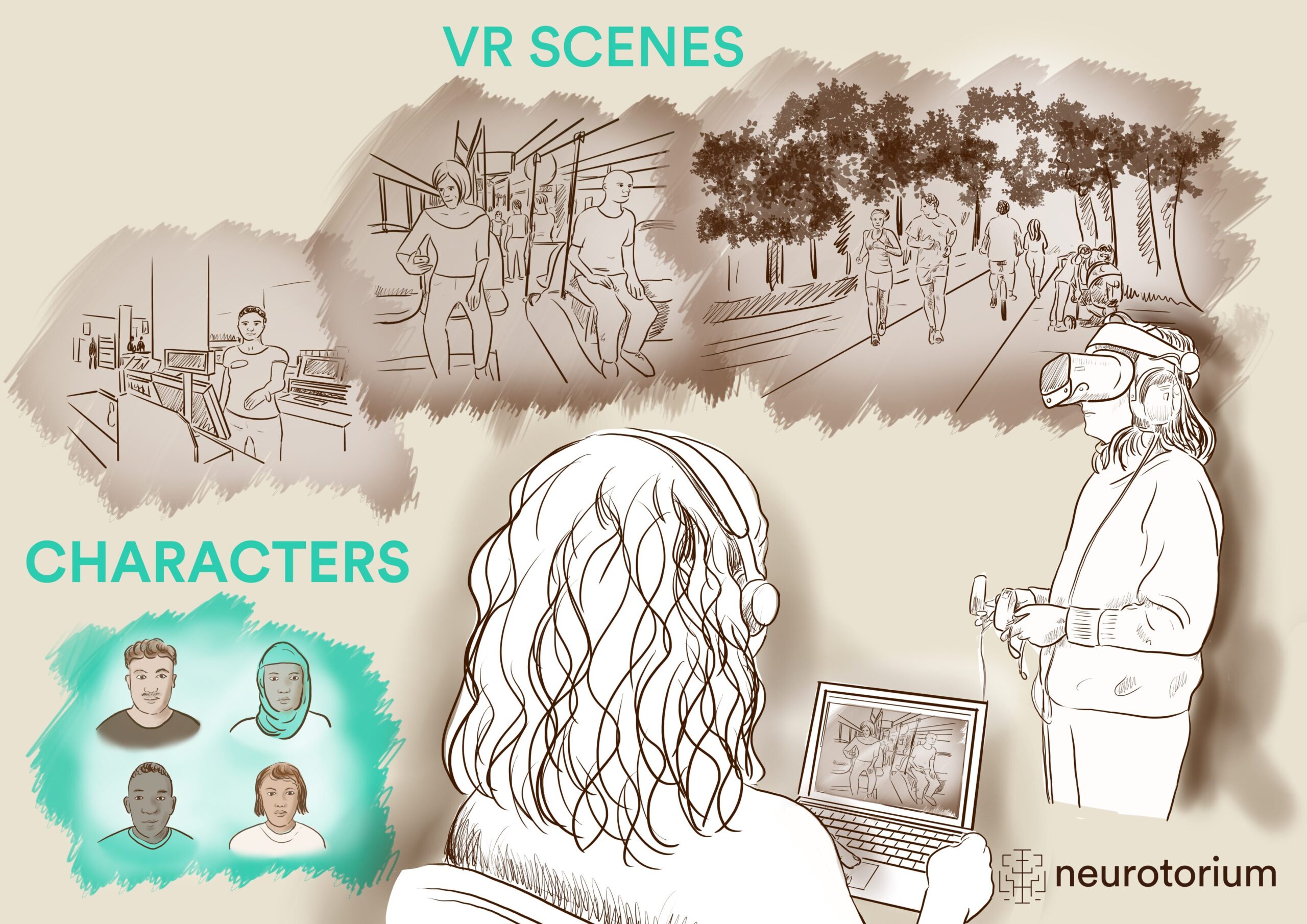
As the lines between virtual and real-world experiences continue to blur, significant therapeutic advances are emerging. In a typical VR intervention, the patient wears a head-mounted display and navigates virtual environments, interacting with objects and avatars using controllers, head movements, and body turns, with sound delivered through headphones. The visual and auditory stimuli are controlled in real-time by a therapist, allowing for highly individualized, gradual, and fine-tuned exposure to triggers of distress.

Figure 1: A virtual reality intervention set-up
VR interventions are generally categorized as either non-immersive (computer-generated 2D environments viewed on a monitor) or semi/full-immersive (3D environments experienced through a head-mounted display), with the latter being more commonly used. Additionally, VR content can consist of either 360-degree videos or animated environments, with the flexibility of animated environments making them the preferred choice for most interventions. It is generally considered a safe intervention with minimal side-effects,3 which typically include motion-sickness or dizziness.
Initially used primarily for anxiety disorders, recent years have witnessed an increasing number of studies exploring the efficacy and tolerability of VR-based therapies in treating severe mental illnesses such as schizophrenia spectrum disorders. These interventions may offer significant potential for patients whose psychotic symptoms show limited response to pharmacotherapy,4 and could be particularly appealing to younger patients, who are more accustomed to engaging with digital platforms as part of their lives, facilitating transfer of this experience to using VR as part of treatment.
Initially used primarily for anxiety disorders, recent years have witnessed an increasing number of studies exploring the efficacy and tolerability of VR-based therapies in treating severe mental illnesses such as schizophrenia spectrum disorders.
Preliminary evidence of VR-interventions in treating symptoms of psychosis
Most studies to date have been small-scale, typically with fewer than 100 participants, often designed as pilot studies, and only in few instances comprising an active control group. The VR-Interventions are generally brief, ranging from 5 to 18 sessions,5 and are typically therapist-led, utilizing VR to deliver a targeted exposure therapy (e.g., targeting a specific symptom such as hallucinations or paranoia).
Psychotic symptoms
VR-based interventions in psychosis are most commonly used to address auditory hallucinations and paranoia. For auditory hallucinations, avatar-based therapies are widely employed, where patients engage in virtual dialogues with avatars representing the source of their dominant voice. Initially developed for non-immersive platforms,6,7 this therapeutic approach has evolved into fully immersive VR8-11 offering the potential for greater efficacy through a more realistic and ecologically valid experience. Primarily aimed at patients with treatment-resistant schizophrenia spectrum disorders, this approach has shown highly promising results, with large effect sizes in reducing auditory hallucinations in one study (Cohen’s d in the range 1.0 – 1.23)12 when compared to TAU.9 However, when compared to cognitive behavioral therapy (CBT)10,13 no superior effect on auditory hallucinations was observed. It is important to acknowledge key methodological limitations, including relatively small sample sizes (N ranging from 19 to 74) and the absence of blinding for outcome assessors, highlighting the need for further robust evidence in the field.
In treating paranoia, VR interventions are typically delivered within a cognitive behavioral therapy (CBT) framework. Participants are immersed in virtual social environments specifically designed to elicit paranoid thinking (e.g., a train, supermarket, etc.), while CBT techniques are employed to challenge distorted thinking, reduce safety behaviors, and alleviate social anxiety. Studies in this area have reported significant improvements in persecutory delusions and social avoidance, with up to large effect sizes (Cohen’s d in the range 0.2 – 1.3).14-17 It must, however, be noted that one study was a feasibility study with only six participants and no control group,16 while two other studies included a control group, either TAU or a waiting list.15,17 Additionally, the study reporting the largest effect size compared the VR-based CBT to VR-exposure but involved a relatively small sample of 30 participants.17 Therefore, the effect sizes should be interpreted with caution.
In treating paranoia, VR interventions are typically delivered within a cognitive behavioral therapy (CBT) framework.
Negative symptoms
There is a critical need for developing effective treatments for negative symptoms,18 and VR-based interventions may offer particular benefits in this area due to their immersive nature, which can be more engaging than traditional treatments. This engagement may be crucial in addressing core aspects of negative symptoms such as anhedonia, social amotivation and avolition. Although limited to a few pilot studies,19-22 existing research on VR interventions for negative symptoms suggests promise by one study finding a large decrease in negative symptoms (Cohen’s d= 1.17). This approach was, however, not designed and tailored specifically to target negative symptoms and was a pilot study with only 21 participants, that were randomized to either the VR-intervention or a passive VR-experience.20 Only one study has directly addressed negative symptoms using a VR treatment approach. This pilot study, involving 30 participants allocated to either the VR intervention or TAU, found that while the intervention supported patients’ recovery goals (Cohen’s d= 1.48), it did not directly reduce the level of negative symptoms.22
VR-based interventions may offer particular benefits in this area due to their immersive nature, which can be more engaging than traditional treatments.
Cognition and social skills
VR-based interventions offer the potential to train specific daily-life skills s such as grocery shopping, meal preparation, and social interactions, effectively targeting neuro-cognitive and social cognitive abilities. Pilot data with small sample sizes (N in the range 12-21) have indicated that VR-interventions for psychosis can enhance general cognitive function, attention, planning skills, and theory of mind with Cohen’s d values ranging from 0.53 – 1.12 when compared to either passive VR20 or integrated psychological treatment.23,24 However, since two of these studies were non-randomized and all were small-scale pilot studies, the findings should be interpreted cautiously. Additionally, predominantly smaller-scale studies with a sample size in the range of N= 7-91, have explored VR’s impact on social skills and functioning, including job interview techniques, vocational skills, and verbal communication19,25-27 finding that VR-interventions can lead to improvements in these areas (Cohen’s d in the range 0.35 – 2.56),28 with one study additionally demonstrating that these improvements can translate into tangible benefits in patients’ daily lives.25 However, only one study was an RCT comparing VR-based social skills training to traditional social skills training.19 Given the very small scale and uncontrolled nature of the majority of these studies, the findings on VR interventions on improving aspects of social functioning can only be considered hypothesis-generating at this stage.
Clinical implementation of VR-interventions: Are we there yet, or what barriers remain?
As stated, VR-based interventions show promise in alleviating symptoms of psychosis. However, particularly for negative symptoms, cognition, and functioning, the effectiveness of VR-based interventions still needs to be validated through rigorous randomized clinical trials prior to targeting scalability and clinical implementation. Most research has explored VR-interventions as adjunctive treatments rather than standalone therapies. Given that VR interventions are targeted, symptom-specific treatments, they are best utilized as part of a comprehensive psychosis rehabilitation program rather than offered in isolation. Integration into broader therapeutic services is essential for maximizing their effectiveness and providing a comprehensive approach to patient care. When addressing symptoms, such as hallucinations or delusions, VR-exposure can be inherently confrontational posing a risk of strong reactions from patients. This fact underscores the importance of ensuring that VR interventions targeting schizophrenia symptoms are delivered by experienced mental health professionals who receive thorough training and ongoing supervision. Integrating these requirements into routine clinical practice can present significant challenges, due to the often scarce clinical resources. Furthermore, an important focus is to ensure the robustness and user-friendliness of the VR-software to accommodate the demands of a busy clinical environment effectively. Finally, health-care providers’ attitude toward new technologies can present a significant barrier to implementation, and addressing this early on is crucial when developing an implementation strategy.
While most research has focused on the acceptability and efficacy of VR-interventions, studying implementation procedures in clinical practice remains understudied, representing a critical next step in translating VR-therapies from the lab to real-world settings. Additionally, research demonstrating the cost-effectiveness of VR-therapies29 is needed, as this finding would further accelerate implementation efforts by gaining support at the policy-making level.
Most research has explored VR-interventions as adjunctive treatments rather than standalone therapies. Given that VR interventions are targeted, symptom-specific treatments, they are best utilized as part of a comprehensive psychosis rehabilitation program rather than offered in isolation.
| Symptom area | VR-based intervention | Outcomes |
| Psychotic symptoms9,10,13-17 | Auditory Hallucinations: Avatar-based therapies, where patients engage with avatars representing the source of their dominant voice. Paranoia: VR interventions within a CBT framework, where participants engage in virtual social environments designed to elicit paranoid thinking (e.g., a train, supermarket) |
Indications on reduction in auditory hallucinations in treatment-resistant schizophrenia spectrum disorders. Fully powered studies with an active control group are needed to draw more definitive conclusion. Significant improvement in persecutory delusions and social avoidance. |
| Negative symptoms19-22 | VR-based interventions for negative symptoms (e.g., anhedonia and avolition). VR’s immersive nature can engage patients, potentially enhancing psychosocial functioning. | Indication on improvement in negative symptoms and patients’ achieving recovery goals. Data from RCTs are needed. |
| Cognition and social skills19,20,23-27 | VR interventions for daily-life skill training (e.g., grocery shopping, meal preparation, social interactions). | Improvements in general cognitive function, attention, planning skills, theory of mind, and social functioning/social skills. Data from RCT’s are needed. |
Table 1: Summary of findings on VR in treating symptoms of psychosis
Summary
VR-based therapies are considered non-invasive and safe treatment options30 with significant potential for addressing key symptoms of psychosis. Their “gamified” nature may make them more engaging and appealing than traditional psychotherapeutic interventions. However, the current evidence remains limited, highlighting the need for a stronger evidence base. Over the coming years, results from large-scale randomized clinical trials8,31-34 will provide more definitive conclusions on the efficacy of VR interventions in people with psychosis, as well as potential subgroups that are particularly suitable or unsuitable for this treatment approach. Additionally, it is essential to evaluate the long-term durability of the positive effects of VR-based therapies by conducting studies with extended follow-up periods beyond the typical 12–24 weeks, with and without booster sessions.
While VR interventions may show promise in improving symptoms and cognition, an important next step is to also demonstrate their effectiveness in translating these benefits into real-world improvements in daily functioning and quality of life. Furthermore, as with all psychosis treatments, a ‘one-size-fits-all’ approach is unlikely to be effective. Therefore, it is critical to explore factors such as symptom complexity, duration of illness, comorbidities, psychological flexibility etc., which may predict individual responses to treatment. Finally, it will be relevant to examine if patients not selected for research participation and not incentivized will engage with VR-based interventions sufficiently and adhere to the schedule, or if and how much drop-out rates will be a challenge in the clinical care environment.
While VR interventions may show promise in improving symptoms and cognition, an important next step is to also demonstrate their effectiveness in translating these benefits into real-world improvements in daily functioning and quality of life.
Related content

In this video, Professors Lakshmi Yatham, MD., and Christoph Correll, MD. discuss the challenges of differentiating bipolar disorder.

In this video Professor Christoph Correll discusses the challenges with available schizophrenia treatments & what clinicians should keep in mind when considering the emerging treatment options for schizophrenia.

{kind=link}
The table summarizes the high-level clinical characteristics of the existing and newly emerging pharmacological treatments for schizophrenia with at least one positive placebo-controlled trial.