
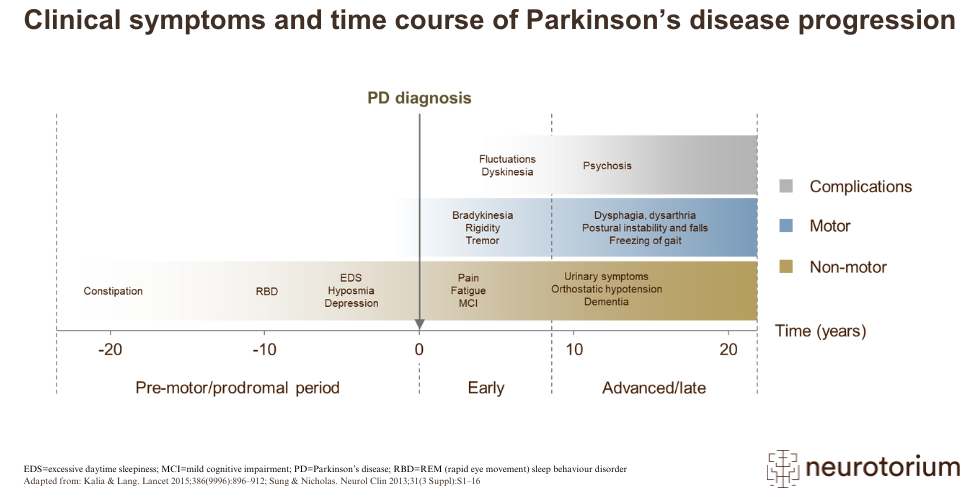
The development of PD is generally slow and progressive.1 While diagnosis tends to occur with the onset of motor symptoms, this can be preceded by a long prodromal phase of 15 years or more.3 This prodromal phase is typically characterised by a range of non-motor symptoms, including sleep disorders, depression, and constipation.3 One of the most common symptoms is ‘REM sleep behaviour disorder’, in which affected individuals can become physically, even violently, active during the REM (rapid eye movement) stage of sleep.1,3
Additional non-motor symptoms develop following clinical diagnosis and, as the disease progresses, cause increasing disability.2 Some symptoms, such as postural instability, dysphagia, and dementia, tend to occur in more advanced disease.1
After several years of levodopa therapy, complications can begin to appear.1 These may include ‘fluctuations’, when patients alternate between periods of good symptom control and poor symptom control.1 In fact, the occurrence of motor response complications (fluctuations and dyskinesias) is one of the main limitations of oral levodopa as a dopamine replacement therapy.1
Related content

Overview of three therapeutic strategies targeting alpha-synuclein in the development of disease-modifying treatments for Parkinson’s disease

Graphical representation of how various treatment strategies can impact disease progression in Parkinson’s disease, from symptom relief to potential cure

{kind=link}
Illustration of how COMT inhibitors increase dopamine availability in Parkinson’s disease by preventing the breakdown of L-DOPA