Index for
slide deck
Introduction
History, definitions and diagnosis
Parkinson’s disease is a chronic, progressive, neurodegenerative condition, mainly affecting the elderly.1
Reference:
1. Lees AJ, Hardy J, Revesz T. Parkinson’s disease. Lancet 2009; 373 (9680): 2055–2066.
The history of Parkinson’s disease
The history of Parkinson’s disease
The ‘shaking palsy’
The condition that we now know as Parkinson’s disease (PD) was first described systematically in 1817 by the London surgeon and apothecary James Parkinson.2,3
In his historic essay, Parkinson drew together his observations of several patients who were affected by similar …
Parkinson’s disease
In 1872, Jean-Martin Charcot identified general slowness of movement (‘bradykinesia’) as a prominent feature of paralysis agitans.1 Bradykinesia is now known as one of the characteristic, or ‘cardinal’, features of PD.1 Charcot also distinguished between the tremors cause…
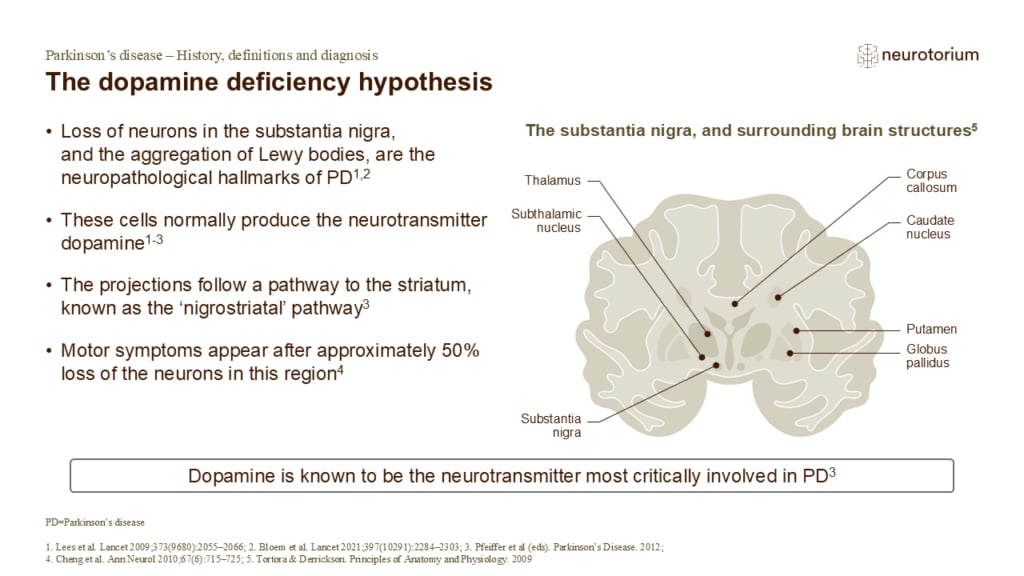
The dopamine deficiency hypothesis
In 1960, scientists showed that brains of PD patients had very low levels of the neurotransmitter dopamine, particularly in the region known as the striatum (comprised of the putamen and the caudate nucleus).6,7 This ‘dopamine deficiency’ appeared to be caused by a marked…
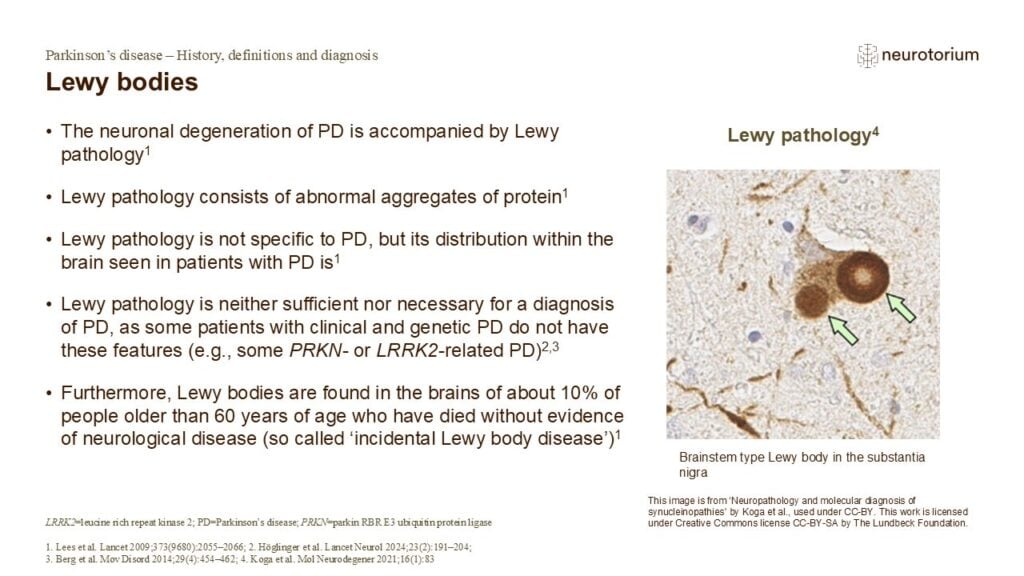
Lewy bodies
Lewy bodies are mostly comprised of abnormal, misfolded protein, and are found in the nerve cells of most patients with PD.1,5 The function of Lewy bodies in the pathogenesis of PD is still unclear, as they have been associated with both neuroprotection and toxicity.6 It …
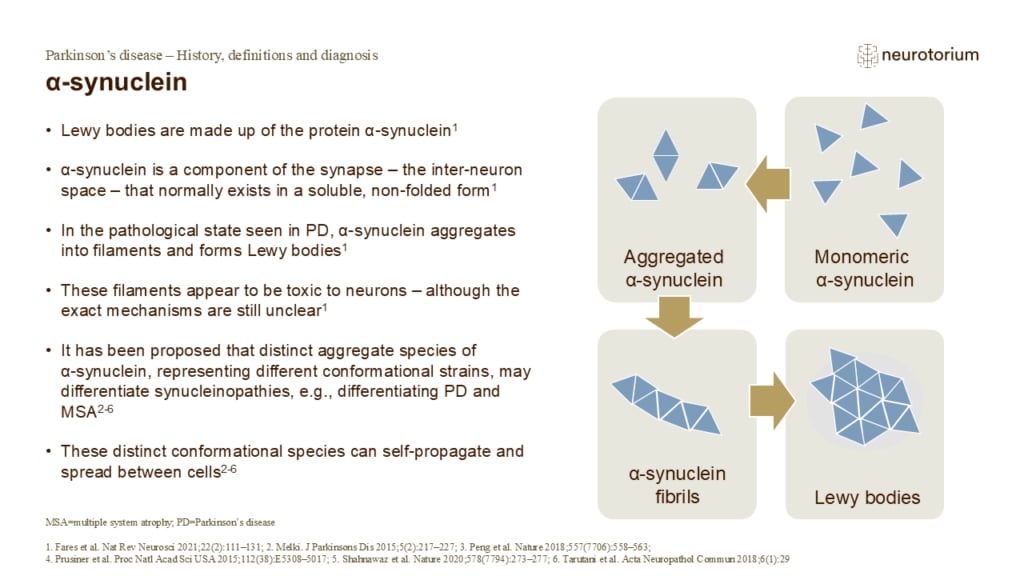
α-synuclein
Since its discovery in the 1990s, the dysfunction of the protein α-synuclein has emerged as a major factor in the development of PD.7 The precise function of α-synuclein has been difficult to determine, but it appears to interact with and affect various proteins at the sy…
The cardinal features of Parkinson’s disease
The cardinal features of Parkinson’s disease
Parkinsonism
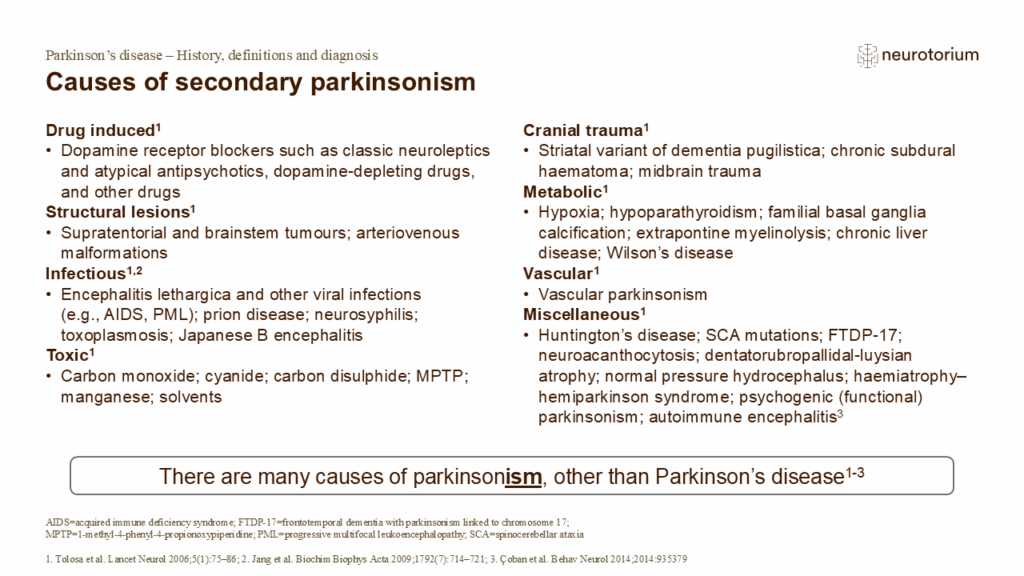
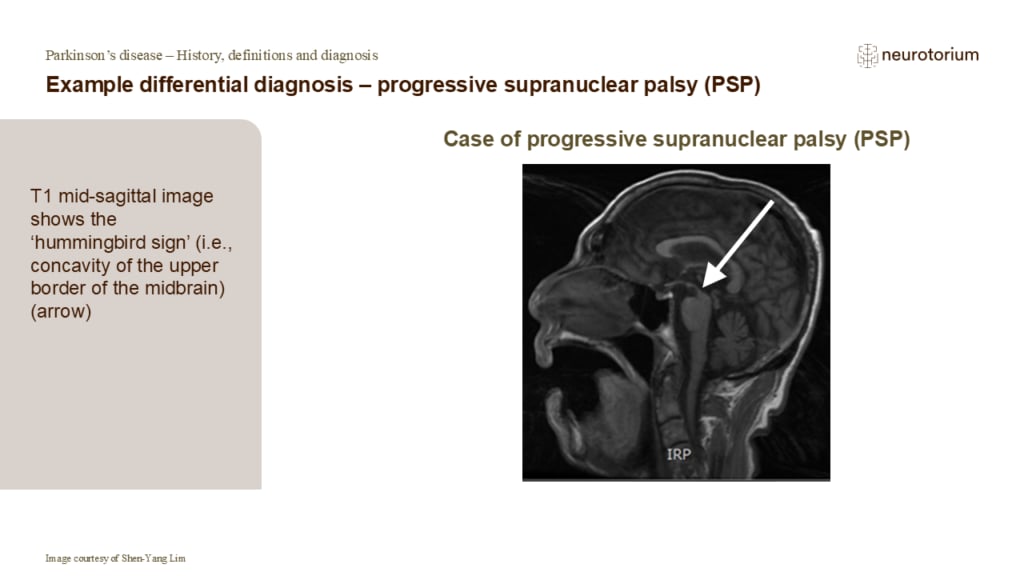
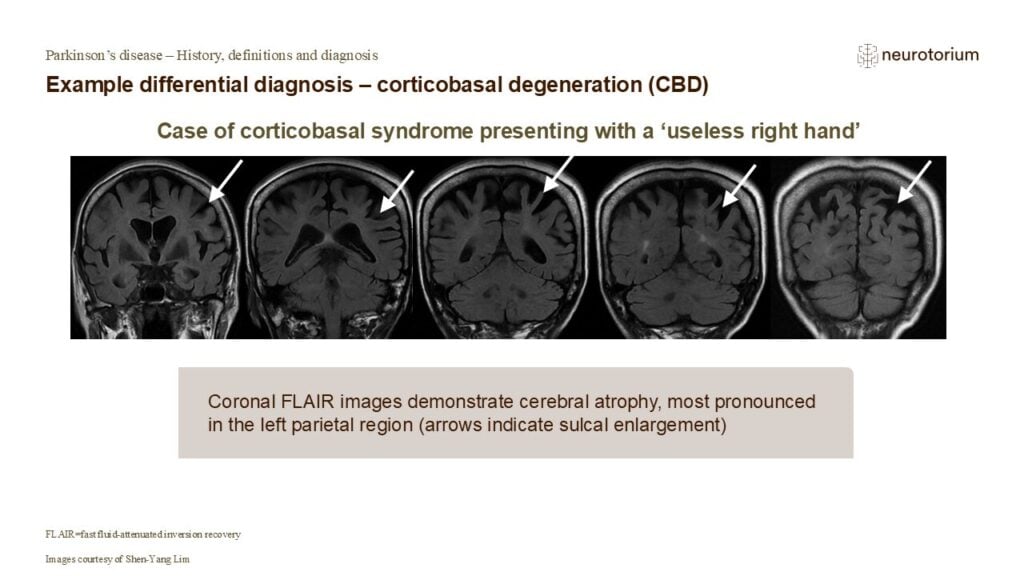
‘Parkinsonism’ is a collection of four clinical features that are typically, although not exclusively, observed in PD.2 The features may also be present in patients with other neurological disorders, including progressive supranuclear palsy, multiple system atrophy, corti…
Motor symptoms – bradykinesia
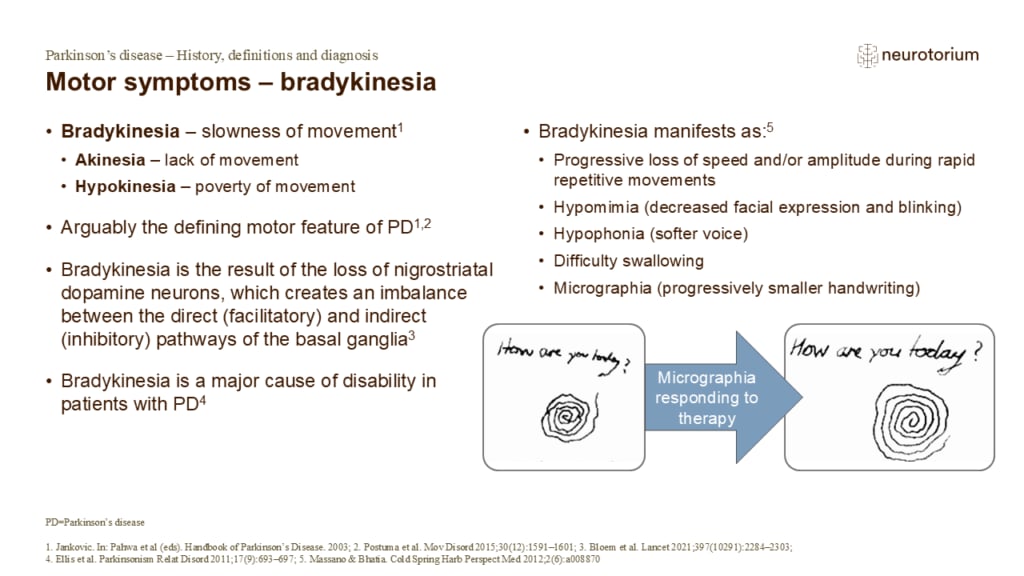
Bradykinesia refers to a slowness of movement.1 Patients with PD often report feeling clumsy or slow, and this may be misinterpreted by family members as a ‘normal’ part of ageing.6 Bradykinesia can manifest in different ways, but it always appears at some point during PD…
Motor symptoms – muscular rigidity
The muscular rigidity or stiffness associated with parkinsonism – sometimes called ‘extrapyramidal rigidity’ – is a key feature of the syndrome.2,3 During the earlier stages of PD, rigidity may manifest solely as pain and can be easily misinterpreted as a musculoskeletal …
Motor symptoms – resting tremor
Tremors are a common and highly-visible symptom of PD, typically present when the patient is fully at rest.5 The shaking action tends to be a rhythmic, medium-frequency oscillation.1 It starts when the particular body part is relaxed and supported by a surface, disappears…
Motor symptoms – postural instability
During the progression of PD, the postural reflexes become increasingly impaired as the brain struggles to integrate sensory information about the relative position of various body parts.3 Since this integration is necessary to maintain balance during movement, the loss o…
Motor symptoms – gait impairment
Postural instability and gait impairments are universally features of advanced PD.1,4 Examination of gait in patients with PD involves asking the patient to stand, unaided, from a seated position, then walk approximately ten metres, turn around, walk back, and sit down ag…
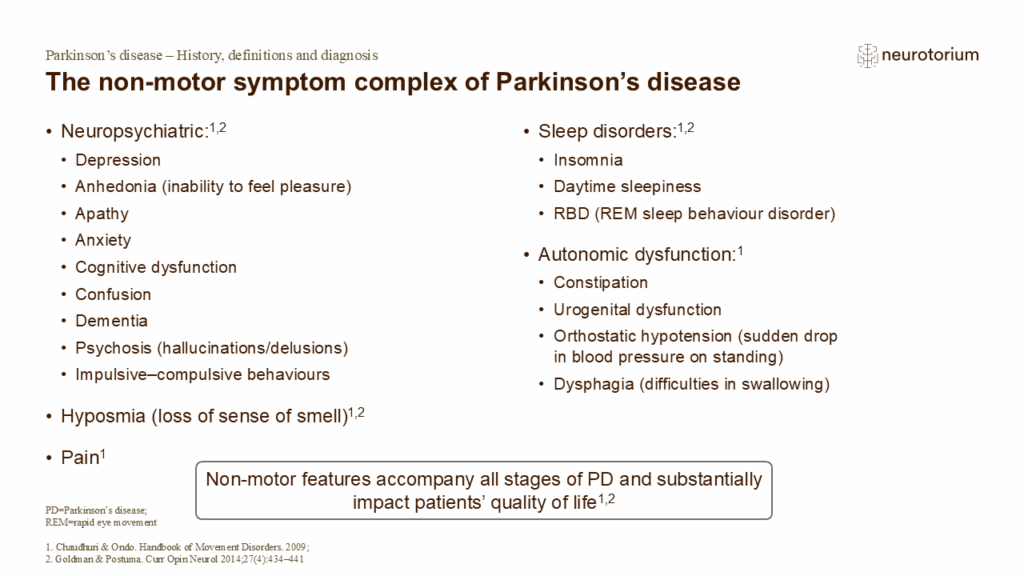
The non-motor symptom complex of Parkinson’s disease
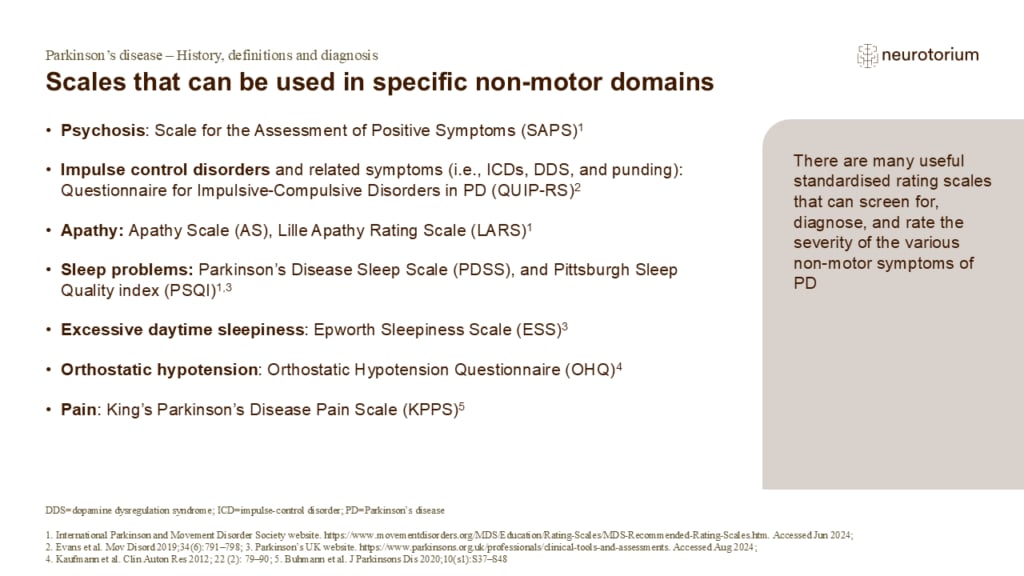
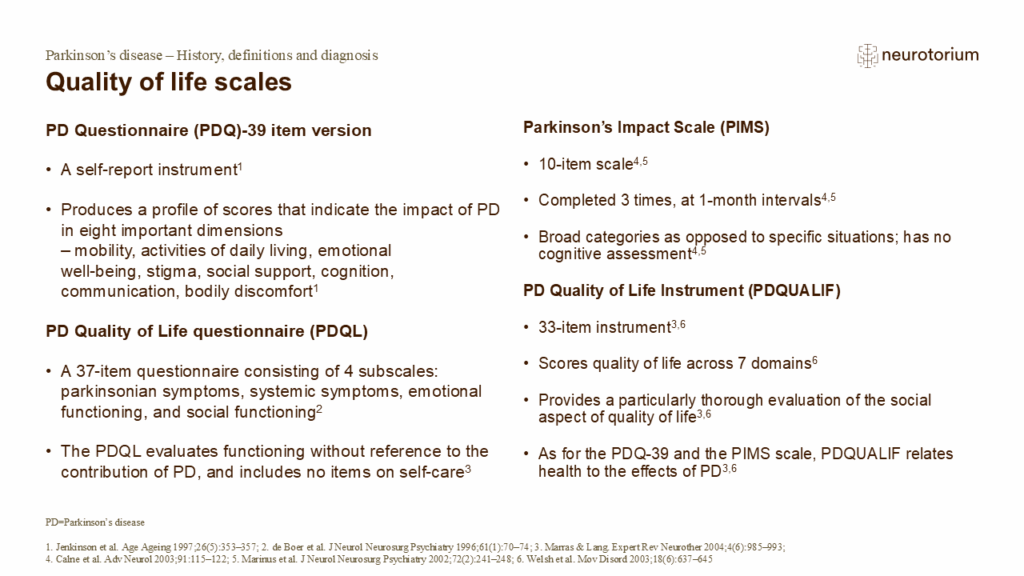
PD has traditionally been regarded as a motor disorder.3 However, physicians are increasingly realising the need to recognise non-motor symptoms, both for diagnostic and management purposes, to try to improve patients’ quality of life.3
Many non-motor symptoms, for exampl…
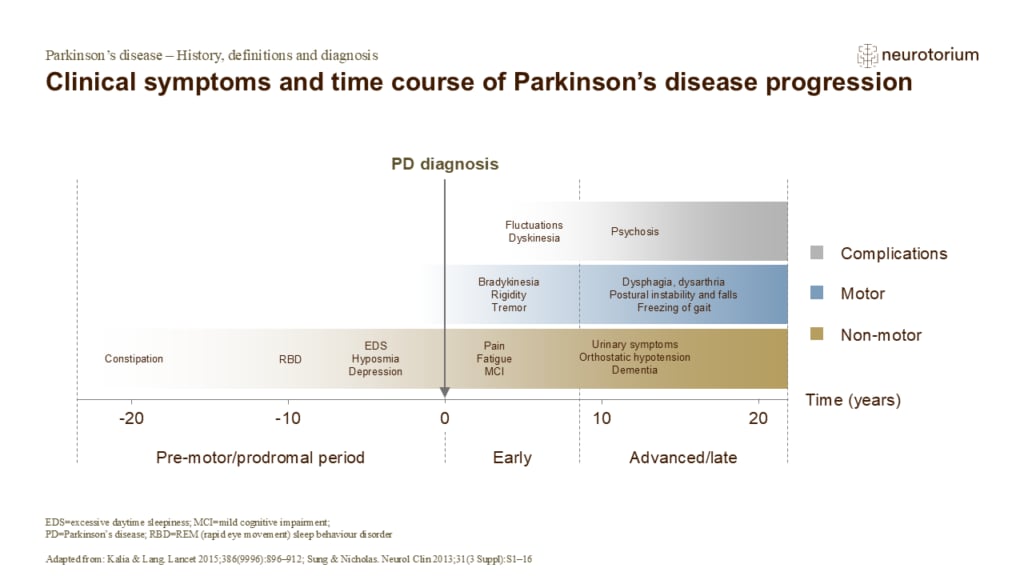
Clinical symptoms and time course of Parkinson’s disease progression
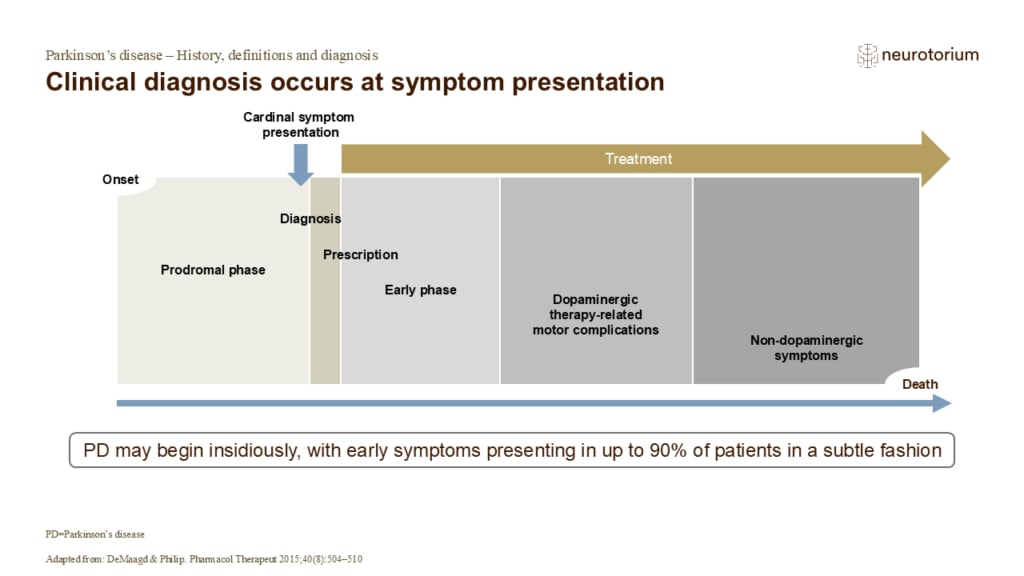
The development of PD is generally slow and progressive.1 While diagnosis tends to occur with the onset of motor symptoms, this can be preceded by a long prodromal phase of 15 years or more.3 This prodromal phase is typically characterised by a range of non-motor symptoms…
Related content
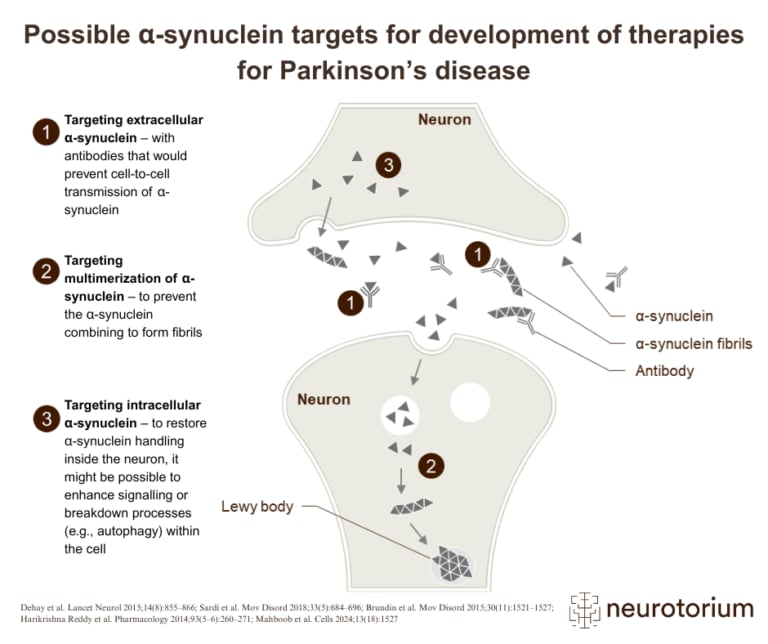
Overview of three therapeutic strategies targeting alpha-synuclein in the development of disease-modifying treatments for Parkinson’s disease
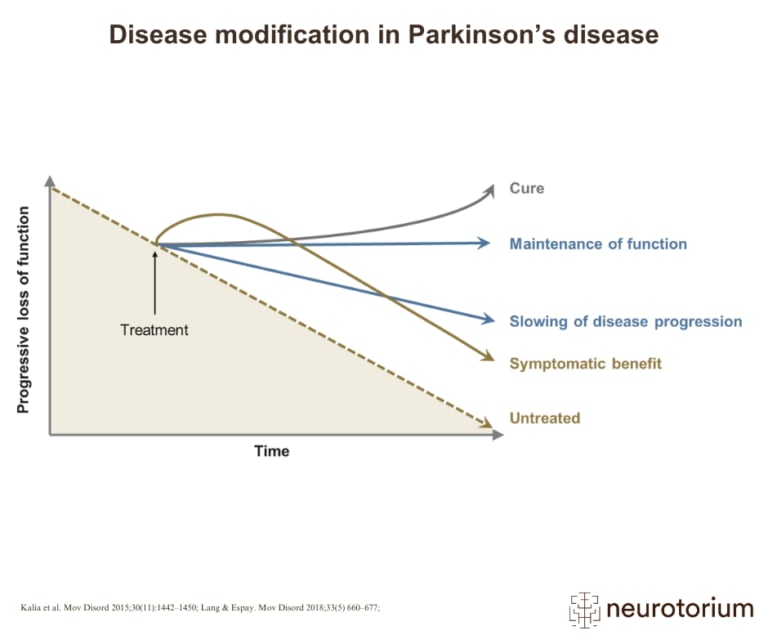
Graphical representation of how various treatment strategies can impact disease progression in Parkinson’s disease, from symptom relief to potential cure
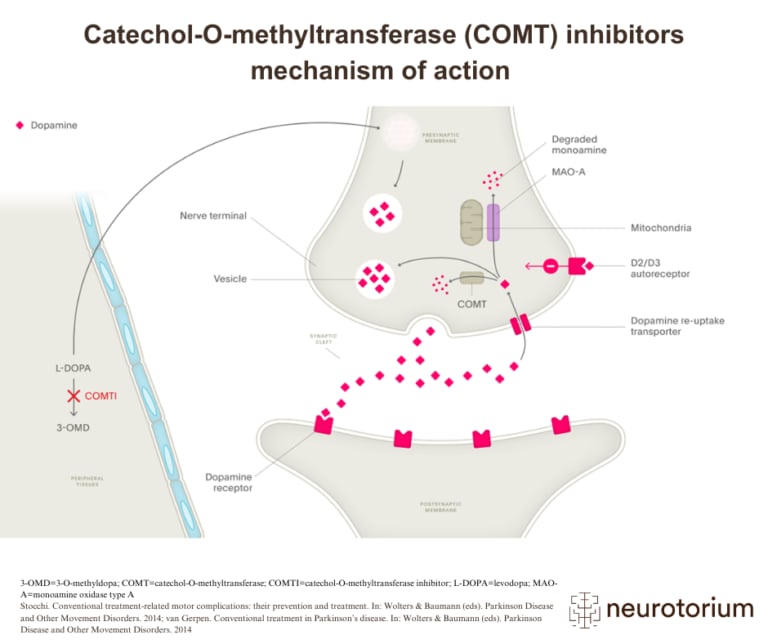
Illustration of how COMT inhibitors increase dopamine availability in Parkinson’s disease by preventing the breakdown of L-DOPA