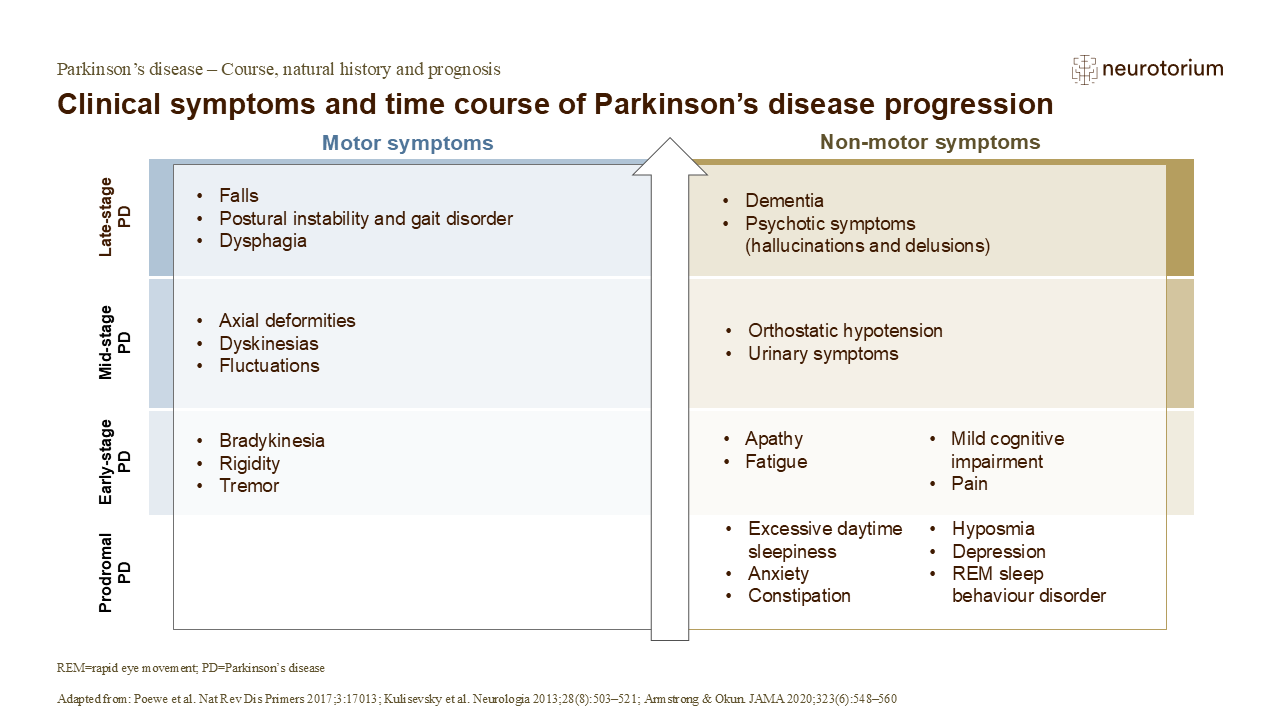
The progression of PD is generally slow, taking place over years (often many years).4 While diagnosis tends to occur with the onset of motor symptoms, this can be preceded by a long prodromal phase of 15 years or more.5 This prodromal phase is typically characterised by a range of non-motor symptoms, including sleep disorders, depression, and constipation.5 One of the most common symptoms is ‘REM sleep behaviour disorder’, in which affected individuals can become physically, even violently, active during the REM (rapid eye movement) stage of sleep.4,5
Additional non-motor symptoms develop following clinical diagnosis and, as the disease progresses, cause increasing disability.4,6 Some symptoms, such as postural instability, dysphagia, and dementia, tend to occur in more advanced disease.4 After several years of levodopa therapy, complications can begin to appear.4 These may include ‘fluctuations’, when patients alternate between periods of good symptom control (ON periods) and poor symptom control (OFF periods).4 The occurrence of these dopa-related response complications remains a major limitation of levodopa as a dopamine replacement therapy.4
Of course, the disease progression experienced by people with Parkinson’s disease in the real world can vary from the typical clinical picture presented above quite appreciably, partly because there are selection biases that arise in clinical research.7 Given that disease modification is a therapeutic goal, a better understanding of real-world disease progression is of critical importance.7
References:
1.Poewe W, Seppi K, Tanner CM, et al. Parkinson disease. Nat Rev Dis Primers 2017; 3: 17013.
4.Kalia LV, Lang AE. Parkinson’s disease. Lancet 2015; 386 (9996): 896–912.