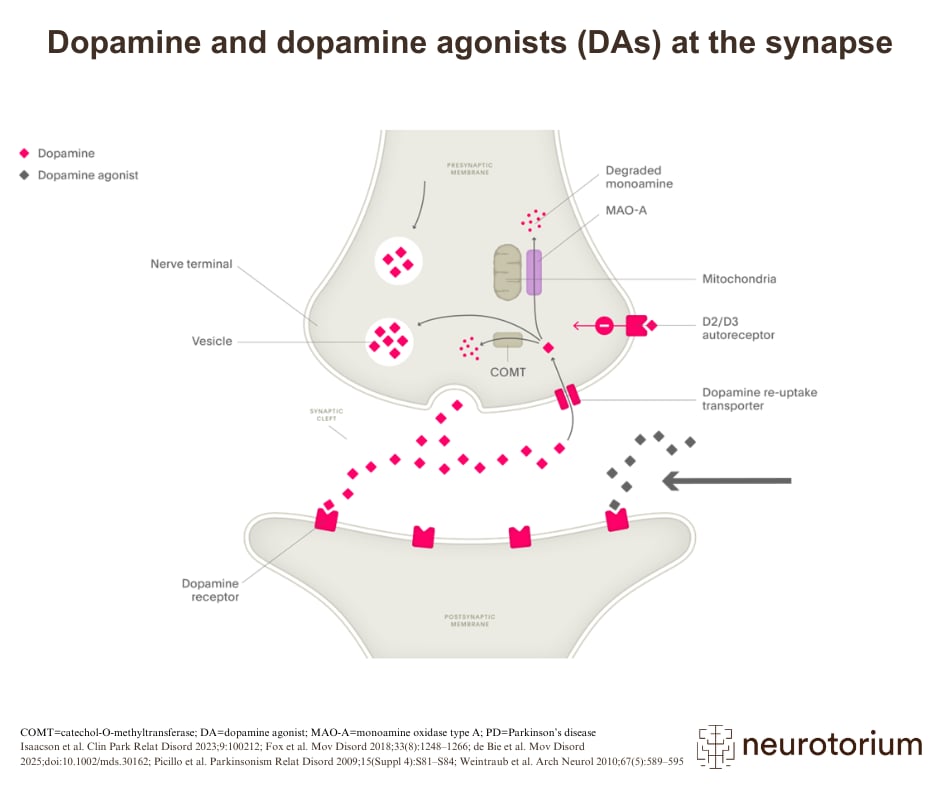
Dopamine agonists play a major role in the treatment of PD.1 They act by directly stimulating intact postsynaptic receptors in the brain linked to motor control.1 Although they tend to be less potent than levodopa in reducing parkinsonian motor symptoms, dopamine agonists are much less likely to cause dyskinesias.1 This characteristic can make dopamine agonists a useful tool for the management of early and fluctuating PD.1
Dopamine agonists have several key advantages over levodopa: they tend to have a longer half-life, which allows for a more prolonged action; their absorption in the gut is not inhibited by dietary protein; and they are easily absorbed across the blood–brain barrier.1 Dopamine agonists may therefore allow the patient to reduce their levodopa usage without worsening their parkinsonian symptoms.2
COMT=catechol-O-methyltransferase; DA=dopamine agonist; MAO-A=monoamine oxidase type A; PD=Parkinson’s disease
Related content
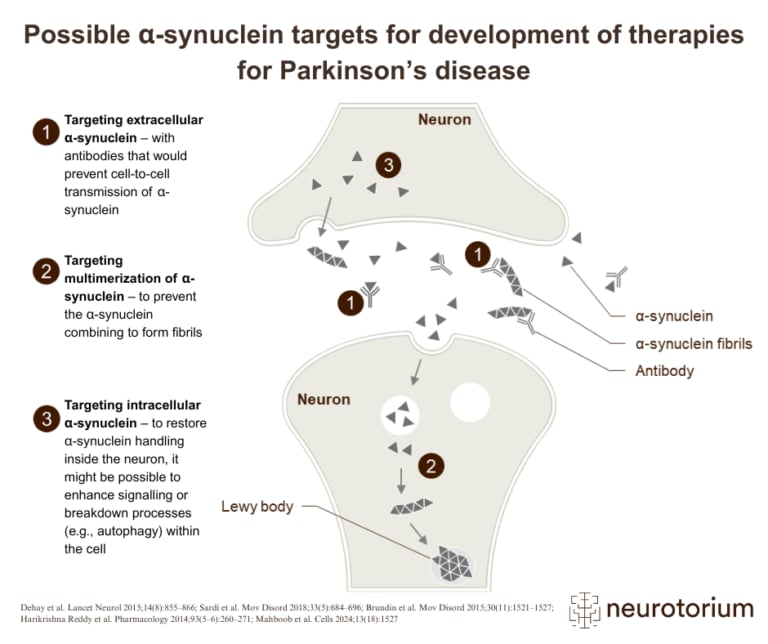
Overview of three therapeutic strategies targeting alpha-synuclein in the development of disease-modifying treatments for Parkinson’s disease
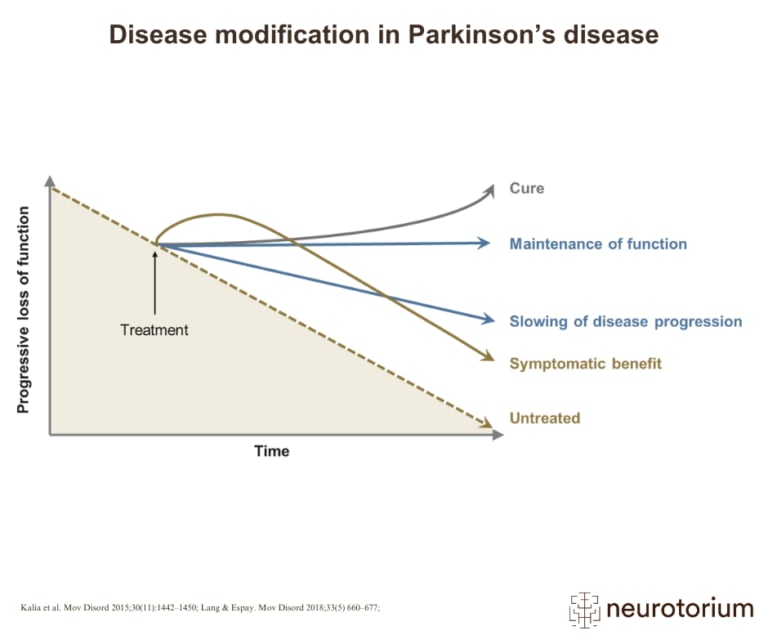
Graphical representation of how various treatment strategies can impact disease progression in Parkinson’s disease, from symptom relief to potential cure
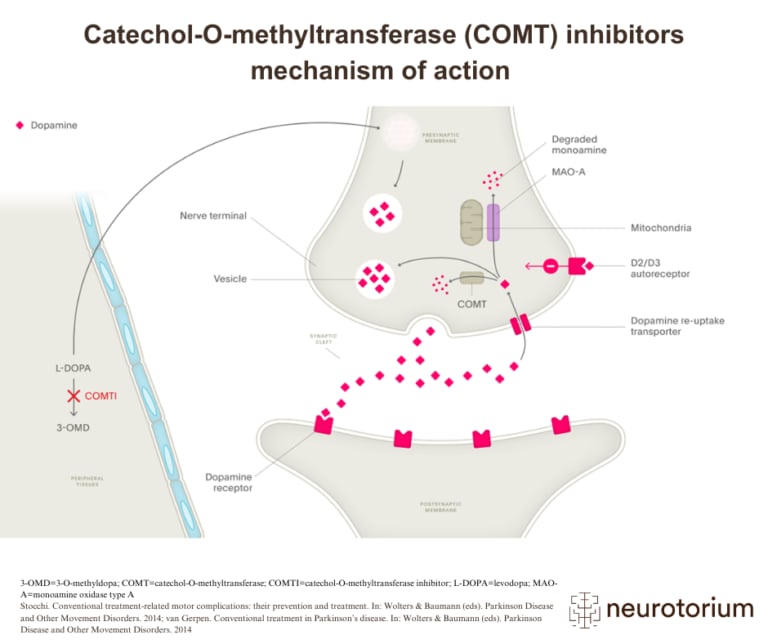
Illustration of how COMT inhibitors increase dopamine availability in Parkinson’s disease by preventing the breakdown of L-DOPA