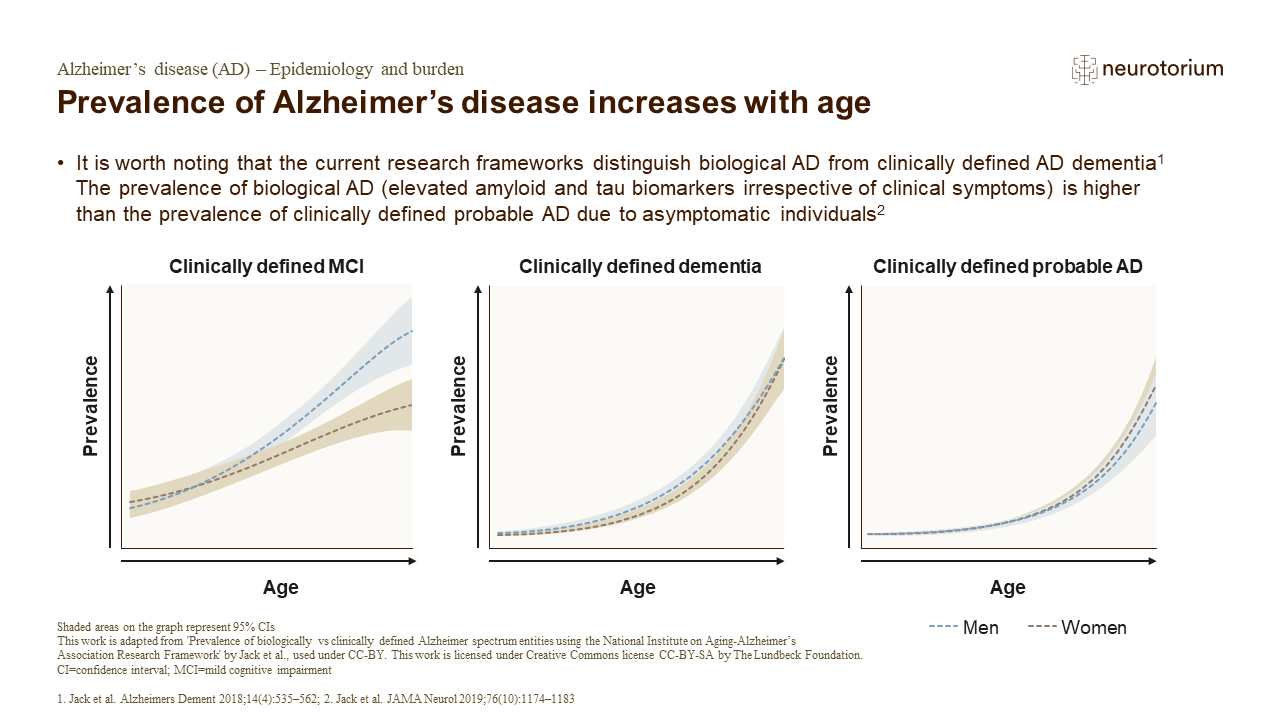
The National Institute on Aging-Alzheimer’s Association (NIA-AA) workgroup recently published a research framework which defined AD by neuropathological or biomarker evidence of amyloid-b plaques and tau tangles, rather than clinical symptoms.1 They then aimed to address the question: ‘what is the prevalence of AD defined biologically using biomarkers compared with the prevalence using conventional definitions based on clinical symptoms?’2 Biologically defined AD entities investigated included Alzheimer continuum, Alzheimer pathologic change, and AD, whereas clinically defined syndromes were mild cognitive impairment (MCI) or dementia, and clinically defined probable AD.2 The study found that the sex- and age-specific prevalence of biologically versus clinically defined diagnostic entities rapidly increased with age, with the exception of Alzheimer pathologic change, which plateaued around the age of 80 in men and women.2 In both men and women, Alzheimer continuum was the most frequent diagnostic entity.2 The prevalence of MCI increases with age, with greater prevalence in men compared with women aged 75 years and older.2 The prevalence of dementia and clinically defined probable AD consistently increases with age, with comparable prevalence in men and women.2
Prevalence of Alzheimer’s disease increases with age