In elderly individuals, AD is the leading cause of dementia, however dementia may arise from a range of aetiologically and neuropathologically distinct disorders that contribute to different patterns of cognitive impairment.1 Understanding these different patterns, and the neurobiological basis of normal and abnormal cognition, has important implications for differential diagnosis.1
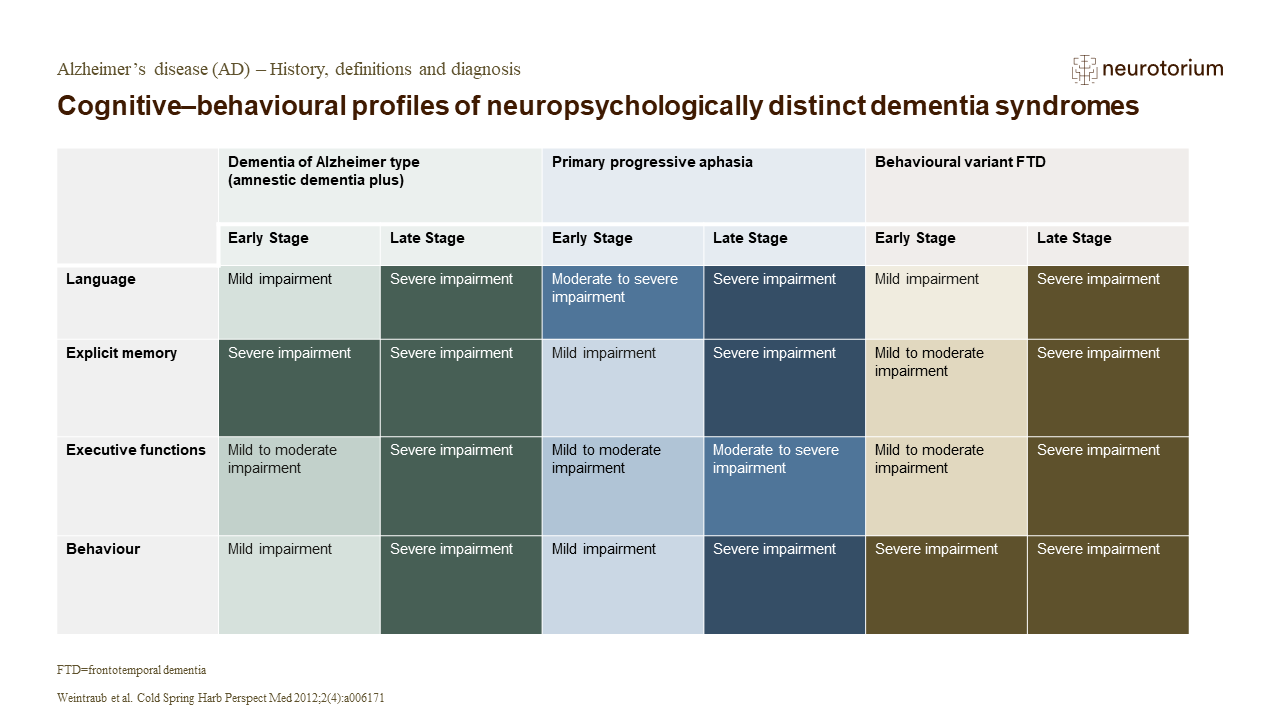
In early stages, it is possible to distinguish domains that are unimpaired or mildly impaired from those that are distinctly abnormal.1 For AD dementia, the most typical early cognitive profile is one of prominent amnesia with additional cognitive deficits.1 In primary progressive aphasia, the early stages are marked in most part by salient language deficits.1 In the early stages of behavioural variant frontotemporal dementia, the most noticeable observations are in the domains of comportment and executive functions.1 The neurological symptoms that present at the very early stages of dementia reflect the neuroanatomical systems that bear the load of the associated pathology, however at these stages, the underlying disease is less obvious.1 While amnestic dementia is most likely to be associated with AD pathology, early aphasia, progressive visuospatial deficits, and changes in personality may also be associated with the neuropathology of AD.1 As dementia progresses from the early to late stages, symptom domain boundaries become increasingly blurred, making distinctive profiles difficult to distinguish.1 Therefore, neuropsychological profiles are most informative during the early stages.1