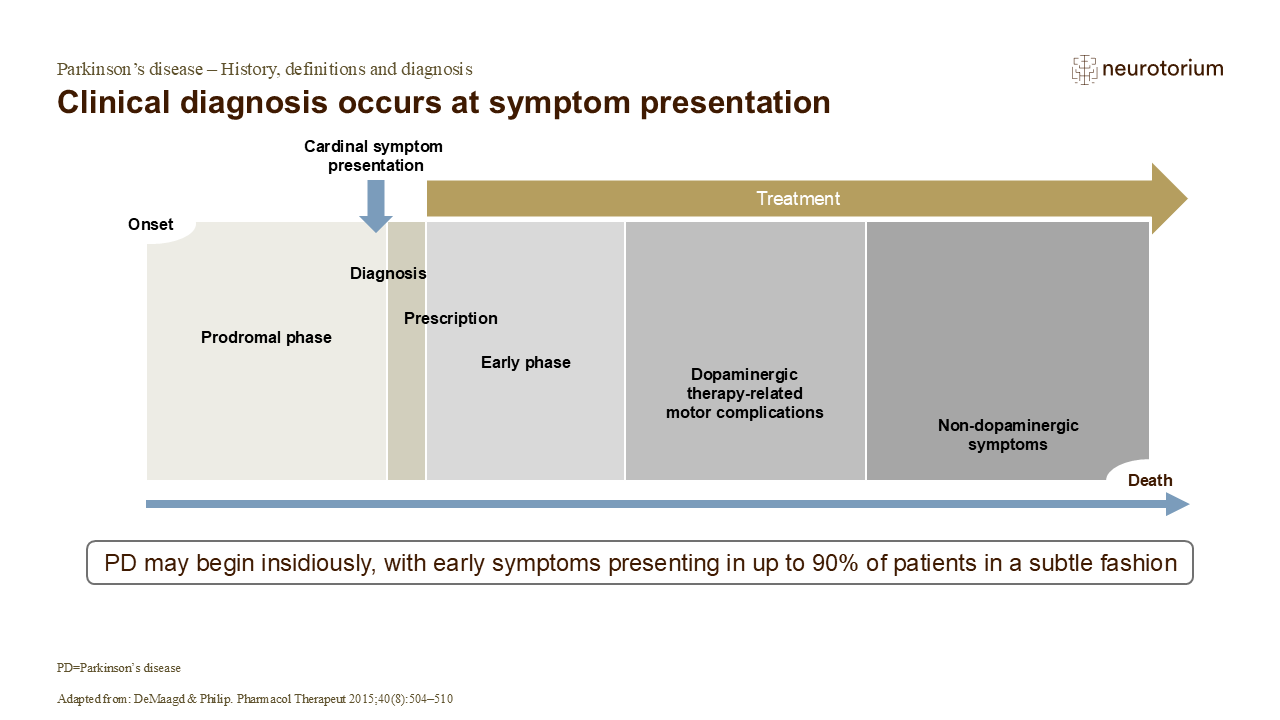
A correct diagnosis of PD allows appropriate forms of therapy and counselling to be made available to the patient.2 As discussed previously, the progression of PD can be subtle at first, manifesting as relatively minor issues, such as experiencing difficulty rising from a chair.1 Typically, younger individuals with PD show less rigidity and bradykinesia compared with older adults, which may delay the accurate diagnosis of their condition.1,3
Diagnosis of PD most commonly occurs on presentation of one or more of the cardinal symptoms, such as bradykinesia, resting tremor, or rigidity.1 In the early stages of the disease, the response to dopaminergic therapy is sustained.4 In the later stages of PD, the loss of neurons in the substantia nigra plus other (e.g., post-synaptic) factors mean that the beneficial effects of each dose of dopamine precursor (levodopa in its formulations) become progressively more short-lived.4
References:
1.DeMaagd G, Philip A. Parkinson’s disease and its management. Pharmacol Therapeut 2015; 40 (8): 504–510.