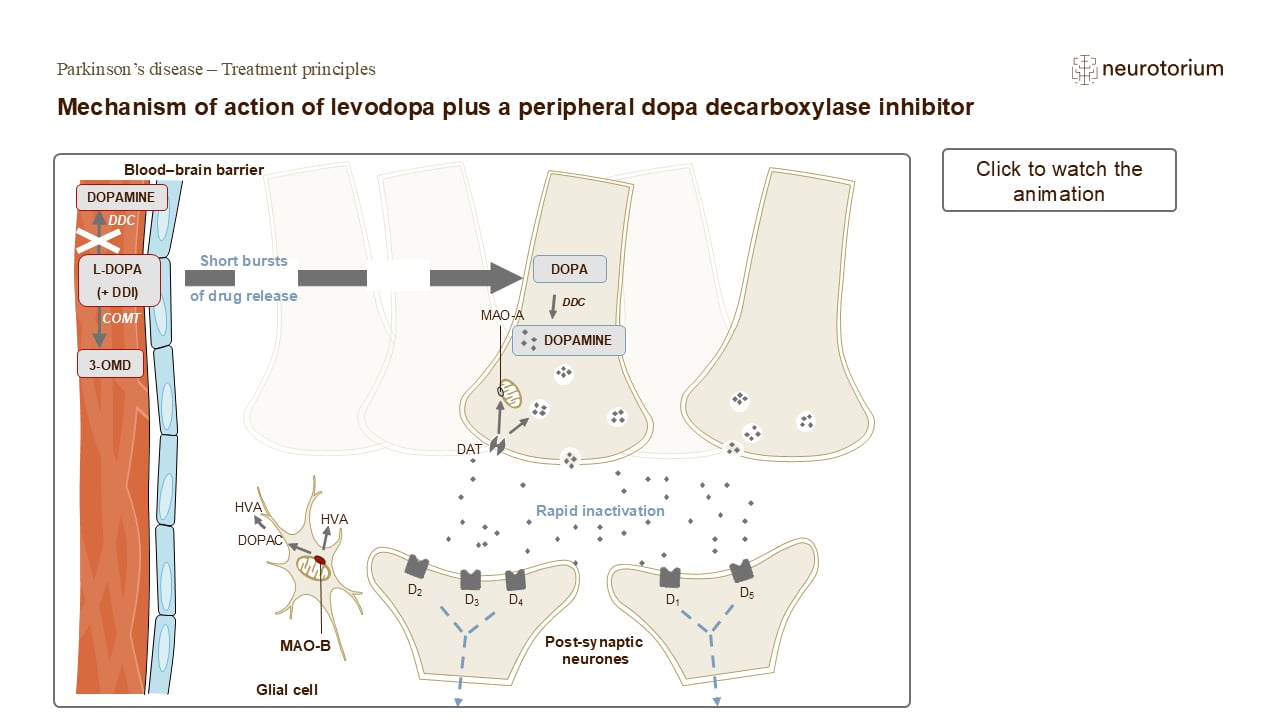
The slide shows the mechanism of action of levodopa, when taken in combination with a dopa decarboxylase inhibitor (DDI). Levodopa can be metabolized to dopamine on either side of the blood–brain barrier.1 It is therefore usually administered with a DDI and with a catechol-O-methyltransferase (COMT) inhibitor to prolong the peripheral levodopa half-life and to increase levodopa availability within the central nervous system.2,3
After passing the blood–brain barrier, levodopa is metabolized by dopa decarboxylase (DDC, also known as aromatic L-amino acid decarboxylase) to dopamine, which is released into the synapse, where it binds to the dopamine receptors (D1, D2, D3, D4 and D5) on post-synaptic neurons.1 Dopamine is then cleared from the synapse either through reuptake into the dopamine neuron by the dopamine transporter (DAT),4 or catabolized by the mitochondrial monoamine oxidase (A or B) into metabolites such as DOPAC (3,4-dihydroxyphenylacetic acid) and HVA (homovanillic acid).5
2. Hauser RA. Levodopa: Past, present, and future. Eur Neurol 2009; 62 (1): 1–8.