


Challenge
Despite a good efficacy of these pharmacological agents approved and recommended for the treatment of anxiety disorders ranging between standardized mean differences (SMDs) of 0.33 and 0.44,2 only ~50% to 67% of patients show an adequate clinical response3. Treatment resistance affecting at least 30% of the patients contributes to a substantial chronicity of anxiety disorders reflected by ranking 6th worldwide among all disorders regarding Years Lived with Disability (YLD) as well as by a high socioeconomic burden and thus poses a significant clinical challenge to the individual patient, the treating physician and society. Additionally, available drugs may not be suitable for every patient due to their adverse-effect profiles, patient preferences, and interindividual biological variability (e.g. genetic and epigenetic factors). Therefore, there is an urgent need for alternative as well as innovative therapeutic options in anxiety disorders.
Off-Label Use
Several drugs such as the antidepressants mirtazapine and agomelatine or the atypical antipsychotic quetiapine are not approved for the indication of anxiety disorders. However, based on either randomized-controlled, open-label studies or case reports, these substances constitute alternative and already available options for the pharmacological treatment of particularly GAD, but also PD or SAD4. For instance, a double-blind, randomized, flexible-dose trial with mirtazapine vs. fluoxetine conducted in a sample of 27 outpatients with PD, mirtazapine proved not to be inferior to fluoxetine and induced a significant clinical improvement. The sleep-improving side effects of mirtazapine might be particularly favorable in anxiety disorders, which are often comorbid with insomnia5. Agomelatine, a melatonin receptor (MT1/MT2) agonist and 5-HT2C receptor antagonist, displayed anxiolytic properties in rodents and was also shown to be effective in the treatment of GAD in several double-blind randomized controlled trials from 12 weeks to 6 months6. Quetiapine has been found effective in GAD in several RCTs, with a recent meta-analysis showing good effect sizes for symptom improvement within the first four weeks7.
Explicitly with respect to treatment-resistant anxiety disorders, RCTs have suggested only very few other substances for (off-label) use as summarized in Table 1, underlining the need for more research into innovative compounds4,8,9.
| GAD | PD | SAD | |
| Antipsychotics | Quetiapine Risperidone Olanzapine |
||
| Antidepressants | Citalopram Clomipramine Paroxetine |
||
| Anxiolytics | Pregabalin | ||
| Anticonvulsants | Clonazepam | ||
| Other | Ketamine | Pindolol | Ketamine |
Table 1: Evidence from randomized-controlled trials (RCT) for (off-label) pharmacological treatment of treatment-resistant anxiety disorders
GAD: generalized anxiety disorder; SAD: social anxiety disorder; PD: panic disorder. Adapted from Domschke et al., 20249 and Schiele et al., 20258.
Pharmacological Pipeline
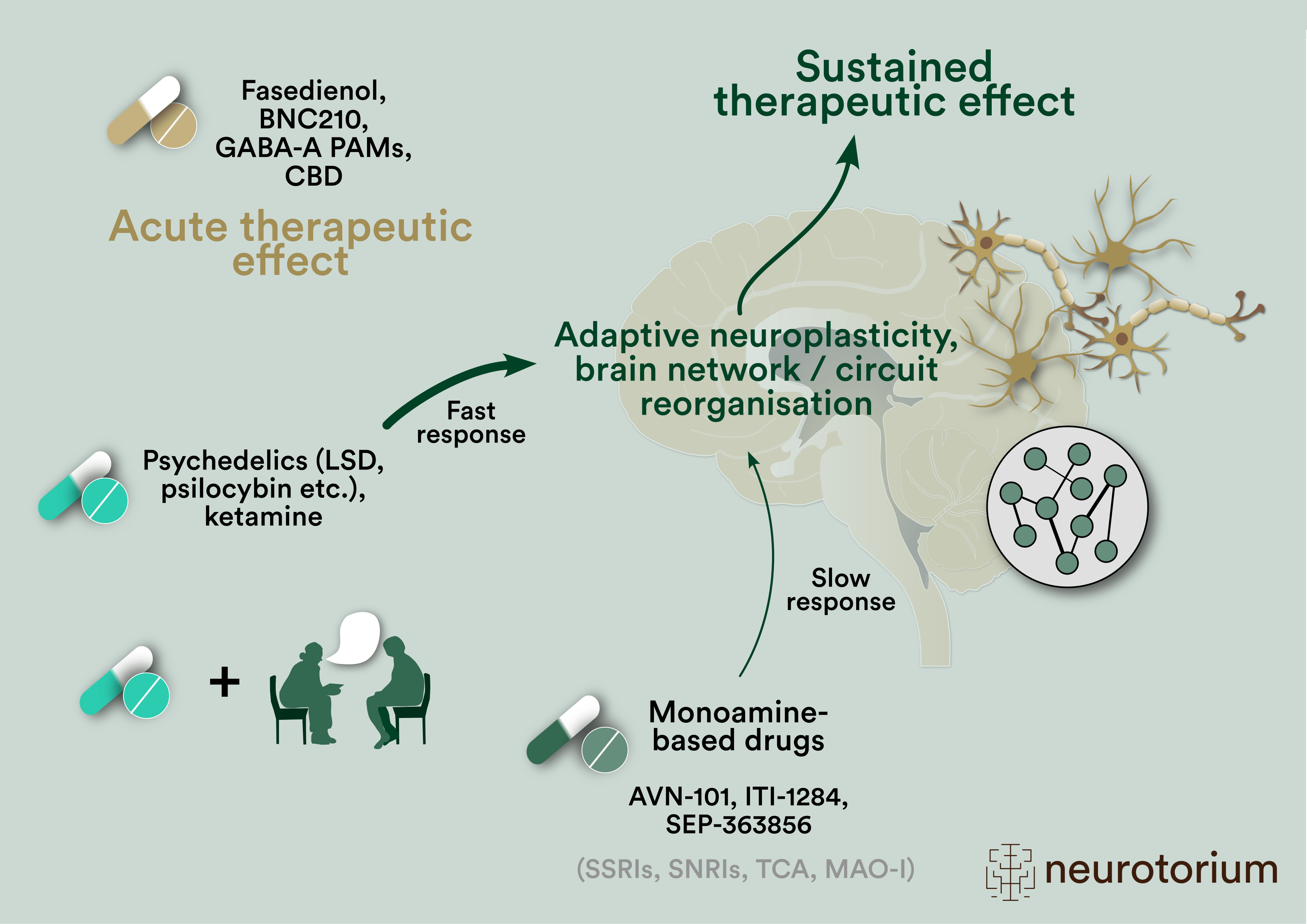
Additionally, novel compounds interacting with classic neurotransmitter systems such as the monoaminergic or γ-aminobutyric acid (GABA)-ergic / neurosteroid systems are currently being refined and further improved. Among those, serotonergic psychedelics such as psilocybin, LSD, CYB004 and the entactogen MDMA, other monoaminergic drugs such as AVN-101, ITI-1284, toludesvenlafaxine, buagafuran or SEP-363856, as well as GABAergic drugs such as ENX-102, darigabat and fasedienol are being explored in the context of anxiety or anxiety disorders. Furthermore, phase I-III studies on substances with novel mechanisms of anxiolytic action targeting for instance the glutamatergic, cannabinoid, neuropeptide or cholinergic systems are being planned or are currently under way, which are listed in Table 2 and exemplarily reviewed below (also see Figure 1) (for a comprehensive review see10,11).
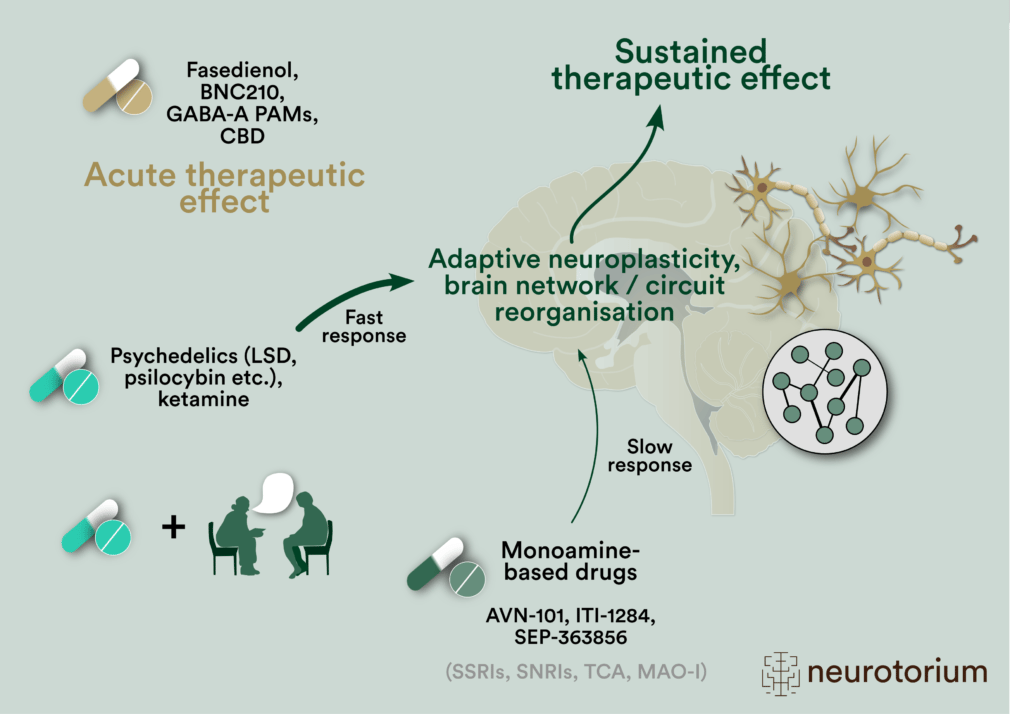
Figure 1: Drugs (selected) in clinical development designed to produce acute and/or enduring therapeutic effects in anxiety disorders. Depicted are also novel drug-assisted psychotherapeutic approaches utilizing neuroplasticity/cognition enhancing effects of drugs.
In grey: existing monoamine-based pharmacological treatment classes.
AVN-101: (CD-008-0045 licenced as AVIANDR in Russia) antagonist at 5-HT2A, 2C, 6 and 7 receptors, adrenergic 2A, 2B and 2C receptors and histamine H1 receptors; BNC210: α7-nAChR negative allosteric modulator (NAM); CBD: cannabidiol; ITI-1284: deuterated form of lumateperone, targets 5-HT2A, D2 receptors and SERT (serotonin transporter); LSD: lysergic acid diethylamide; MAO-I: Monoamine oxidase inhibitors, MDMA: 3,4-Methylendioxy-N-methylamphetamin; PAMs: positive allosteric modulators of the GABA-A receptor; SEP-363856: 5-HT1A receptor and TAAR1 (trace amine-associated receptor 1) agonist, SNRIs: serotonin and noradrenaline reuptake inhibitors, SSRIs: serotonin reuptake inhibitors, TCA: tricyclic antidepressants.
Psychedelics
Much attention is currently being paid to the investigation of psychedelics such as LSD or psilocybin, which have been hypothesized to exert long-term effects by rapidly and lastingly stimulating neuroplasticity12,13.
LSD is a classic psychedelic substance that interacts as a partial agonist with the serotonin 5-HT2A receptor. A double-blind, placebo-controlled, randomized crossover design with two LSD (200 µg) and two placebo sessions and five study visits per period enrolled 42 patients >25 years, with a DSM-IV diagnosed anxiety disorder associated or not with a somatic illness. LSD led to a significant reduction in anxiety compared to placebo in the first treatment period. The maximum effect was achieved two weeks after the second LSD session and lasted up to 16 weeks14. Furthermore, LSD tartrate (MM120) investigated in phase III multicenter RCTs for GAD (NCT06741228, VOYAGE, NCT06809595, PANORAMA) received FDA breakthrough designation.
Much attention is currently being paid to the investigation of psychedelics such as LSD or psilocybin, which have been hypothesized to exert long-term effects by rapidly and lastingly stimulating neuroplasticity12,13.
GABA / Neurosteroid Systems
GABAergic signaling has been identified as one particular potential mechanism underlying anxiety disorder genetic risk and has been the main target for licenced drugs with acute anxiolytic action. Benzodiazepines act as positive allosteric modulators (PAM) of the GABA-A receptor. Dose-dependent side effects such as sedation, motor impairment, as well as dependence led drug development to design novel GABAkines – compounds which act at specific GABAA-receptor subunits and thereby promoting anxiolytic effects while minimizing side effects15. Phase II trials for the α1 sparing, α2/3/5-selective GABAA-receptor PAMs ENX-102 and darigabat are currently underway for GAD and PD, respectively16.
Another class of drugs acting as endogenous GABAA-receptor PAMs are neuroactive steroids (neurosteroids). The neurosteroid fasedienol (aloradine) is proposed to act as a vomeropherine to activate olfactory bulb neurons connecting to emotion-regulating areas of the brain. After showing rapid-onset beneficial effects against SAD symptoms in a randomized, multi-center study, these results are being followed-up in current phase III trials for SAD (PALISADE 3 and 4, NCT06615557) delivering fasedienol in aerosol form as a nasal spray.
In this video, Professor Nicolas Singewald discusses the emerging opportunities and challenges associated with pharmaceutical treatments for anxiety disorders. Anxiety disorders are the most prevalent psychiatric conditions, with no new drug approvals in decades. Current treatments, such as benzodiazepines and SSRIs/SNRIs, have significant side effects and limited efficacy, with around 1/3 of patients not responding adequately. Research is exploring novel targets like cholinergic, glutamatergic, and endocannabinoid systems, as well as psychedelics and multimodal drugs. Promising candidates include rapidly acting anxiolytics, neurosteroids, and ketamine/CBD. The focus is on enhancing neuroplasticity and developing personalized treatments based on neurobiological heterogeneity, with ongoing efforts to establish reliable biomarkers for patient subtyping.
Glutamate System
Ketamine, a voltage-dependent NMDA glutamate receptor antagonist, appears to offer rapid and sustained anxiety symptom relief across a range of clinical settings, with anxiolytic effects occurring within the first 12 h of administration and remaining effective for 1-2 weeks17. Regarding the use of ketamine in anxiety disorders as categorical entities, ongoing studies are addressing SAD and GAD. Only two small randomized controlled studies in SAD are completed to date18. A meta-analysis of these very small studies showed a significant superiority of ketamine at a dose of ≥0.5 mg/kg body weight over placebo19. These initial findings warrant validation in large samples before clinical relevance can be derived.
Cannabinoid System
While the endocannabinoid system – comprising e.g. the two major endocannabinoids anandamide and 2-arachidonylglycerol, the endocannabinoid receptors CB1/2 and the degrading enzyme fatty acid amide hydrolase (FAAH) – is being intensively researched pre-clinically in the context of anxiety, to date there is no sufficient evidence from randomized controlled studies for the use of cannabis or its derivates in the treatment of anxiety disorders20,21.
Preliminary evidence has been provided for cannabidiol augmentation (200-800 mg/day) in patients (15-25 years of age) with any treatment-resistant anxiety disorder22. Cannabidiol (300 mg) as an augmentation strategy to enhance in vivo exposure therapy in SAD and PD, however, did not prove to be effective in a recent RCT23. Currently, cannabidiol is investigated in several anxiety disorders24,25, for instance in SAD (NCT05600114), in GAD, SAD or PD (NCT03549819), or regarding its potential for augmenting fear extinction in SAD (NCT06123702). Finally, ONO-1110, a cannabinoid modulator with limited published pharmacological details, is investigated in SAD (NCT06805565).
Neuropeptide Systems
Several neuropeptides such as oxytocin, orexin, neuropeptide Y (NPY), corticotropin releasing hormone (CRH), vasopressin, substance P, cholecystokinin or neuropeptide S (NPS) have preclinically been suggested to represent potential targets of drug development in the field of anxiety disorders26,27. However, only oxytocin is currently targeted in clinical trials (e.g., NCT05968651).
Cholinergic System
The α7-nAChR negative allosteric modulator, BNC210, has been shown to reduce anxiety and stress-related behavior and to increase fear extinction in animal models28. Clinically, small studies show reductions in self-reported anxiety (STAI) in individuals with GAD and decreases in amygdala responses to threat (fearful faces) (for a review see 29). BNC210 has been fast-tracked by the FDA and is currently being investigated in a phase III study (AFFIRM-1) as an “acute as-needed treatment” of anxiety in SAD.
| Targets | GAD | PD | SAD | Anxiety |
| Psychedelics and MDMA | MM-120 (LSD) (III)
Psilocybin (II) CYB004 ((II) |
MDMA (II)
EMP-01 (II) |
Psilocybin (I-II) | |
| Other monoamine systems
(5-HT, NA, DA) |
AVN-101 (III)
ITI-1284 (II) Buagafuran (III) SEP-363856 (II/III) Toludesvenlafaxine (III) |
|||
| GABA / neurosteroid systems | ENX-102 (II) | Darigabat (II) | Fasedienol (III) | |
| Glutamate system | Ketamine (II) | Ketamine (II) | Ketamine (I) | |
| Cannabinoid system | Cannabidiol (III) | Cannabidiol (III) | Cannabidiol (III)
ONO-1110 (II) |
Cannabidiol (II) |
| Neuropeptide system | Oxytocin (II) | Oxytocin (II) | ||
| Cholinergic system | BNC210 (III) | |||
| Nutraceuticals | HB-1 (II) |
Table 2: Overview of compounds in clinical development for the treatment of anxiety disorders
The phase of clinical development (I-III) of each compound is provided in brackets. Bold lettering depicts compounds that have received breakthrough or fast-track designation by the FDA (United States Food and Drug Administration agency). Updated from Singewald et al., 2023 10 and Zwanzger et al., 202136.
Abbreviations and explanations: 5-HT: serotonin; AVN-101: (CD-008-0045 licenced as AVIANDR in Russia) antagonist at 5-HT2A, 2C, 6 and 7 receptors, adrenergic 2A, 2B and 2C receptors and histamine H1 receptors; BNC210: α7-nAChR negative allosteric modulator (NAM); buagafuran is a derivative of agarofuran, which was extracted from Aquilaria agallocha Roxb., interacts with monoamines and neuronal delayed rectifyer potassium channels; CYB004: deuterated dimethyltryptamine (DMT); DA: dopamine; EMP-01: R-enantiomer of MDMA; ENX-102: GABA-A ɑ2,3,5 PAM, blocks ɑ1 (ENCALM study); GABA: g-aminobutyric acid; GAD: generalized anxiety disorder; HB-1: nutraceutical of undisclosed composition; ITI-1284: deuterated form of lumateperone, targets 5-HT2A, D2 receptors and SERT (serotonin transporter); LSD: lysergic acid diethylamide; MDMA: 3,4-Methylenedioxy-N-methylamphetamine; MM-120: LSD D-tartrate; NA: noradrenaline; ONO-1110: cannabinoid modulator; PD: panic disorder; SAD: social anxiety disorder; SEP-363856: 5-HT1A receptor and TAAR1 (trace amine-associated receptor 1) agonist; toludesvenlafaxine (ansofaxine) is a triple (5-HT, NA, DA) reuptake inhibitor.
Outlook
Currently, there is promise in the refinement of existing as well as the development of innovative compounds to tackle the clinical challenge of treatment resistance in anxiety disorders. These efforts also include novel drug-assisted psychotherapeutic approaches utilizing neuroplasticity/cognition enhancing effects of drugs. Still, further studies are warranted to explore potentially druggable targets in even more experimental, future-oriented fields. For instance, epigenetic mechanisms such as histone modifications – positioned at the interface of the environmental and the genetic level – have been suggested to be crucially involved in the pathogenesis of anxiety disorders30. Accordingly, pre-clinical studies imply that increasing histone acetylation, either via genetic or pharmacological inhibition of histone deacetylases (HDAC), augments fear extinction and protects from return of fear phenomena. Thus, it might be worthwhile to develop relevant subtype-specific HDAC inhibitors and clinically investigate them as pharmacological adjuncts to augment the efficacy of exposure-based approaches in anxiety disorders31. Other approaches looking at extinction augmentation comprise for instance studies on D-cycloserin (DCS), a NMDA glutamate receptor glycine site partial agonist, which has been suggested to facilitate fear extinction both in preclinical and clinical studies in patients with specific phobia, SAD and PD with or without agoraphobia32. Psychedelics, MDMA, cannabinoids, L-DOPA or more recently Losartan, a commonly prescribed blood pressure drug targeting the renin-angiotensin system (NCT06636812), are also being explored in this context. Additionally, anti-inflammatory treatment approaches such as microglia-directed treatments, pro-inflammatory cytokine inhibitors, COX-inhibitors, phytochemicals and a number of novel anti-inflammatory agents might constitute novel alternative or complementary therapeutic options in specific “inflammatory” subtypes of anxiety disorders33. Also, while currently available evidence for a role of the microbiome in anxiety disorders is limited, randomized-controlled trials in clinical populations are warranted to elucidate the potential of probiotics targeting the microbiome in reducing anxiety symptoms34. Finally, biomarkers – once robustly identified and validated – will inform a more personalized, individually tailored and thus more effective treatment of anxiety disorders35.
Currently, there is promise in the refinement of existing as well as the development of innovative compounds to tackle the clinical challenge of treatment resistance in anxiety disorders.
Related content
{kind=link}
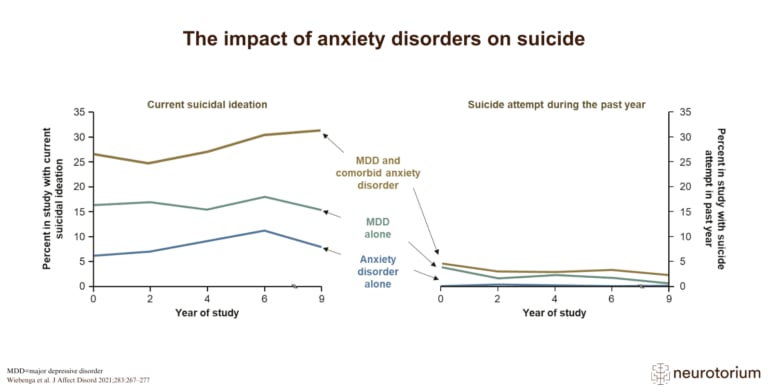
Suicidal ideation is far more common than attempts in people with anxiety or depression, especially with comorbid disorders and severe depression.