

Epilepsy is a long-recognized condition described in some of the oldest written works dating back to Mesopotamia in 2000 BC.1 With the notable exception of Hippocrates, most early descriptions of epilepsy ascribed the disorder to supernatural causes, including biblical descriptions of demonic possession.i In this context, it is not surprising that a person with epilepsy (PWE) was considered a threatening entity. But fear, rejection, and “othering”ii of people living with epilepsy continues to be a major additional burden, a burden beyond seizures, for many people globally. Because of the substantial negative impact epilepsy-associated stigma can have upon persons with epilepsy and their loved ones, recognizing this social phenomenon, with its myriads of manifestations, is important for clinicians, medical educators, policy makers, and community leaders.
(i) Matthew 17:14-18, Mark 9:17-27, Luke 9:37-43
(ii) Othering: A social process through which individuals and groups are marginalized by being defined as different and inferior to a perceived dominant social norm.2
Definitions and Measures
Felt stigma entails anticipating negative perceptions of oneself from others due to a ‘spoiled identity’.iii Self-stigma occurs when those negative perceptions are internalized. Enacted stigma is when actual discrimination occurs as a result of stigmatizing beliefs and attitudes.
Quantifying stigma is important for understanding the relative burden of epilepsy-associated stigma and risk factors for stigma. One can quantify the experience of being stigmatized and/or the extent or degree of the potential stigmatizer’s negative attitudes, beliefs, or practices, where stigmatizing practices are essentially acts of discrimination. The table below provides a framework to consider how stigma is usually quantified. A few example instruments are listed, but there are many more. These instruments or similar ones were used in research that informed the identification of factors that increase (or decrease) the risk or burden of epilepsy-associated stigma.
(iii) When some is reduced from a whole or usual person to a tainted or discounted one because of a negative attribute, this results in a spoiled identify, reducing them from a whole and usual person to a tainted and discounted one. This spoiled identity affects how others perceive and interact with the individual, impacting their social acceptance and opportunities. 3
| To evaluate potential stigmatizers | |
| Instruments | Sample items |
| Epilepsy stigma scale (10 items)4
Stigma scale of epilepsy (24 items) Knowledge, attitude, belief and practices instruments5 |
|
| To evaluate persons living with epilepsy | |
| Instruments | Sample items |
| Jacoby’s 3-item stigma scale6
Stigma scale of epilepsy (24 items)7 Kilifi stigma scale for epilepsy8 |
Designed to quantify felt stigma
|
Table 1: Framework for Measuring Stigma
This table provides examples of instruments appropriate for measuring stigma based upon who the instrument would be delivered to (a PWE vs a possible stigmatizer) as well as sample items included in the instrument. Note that the list is not exhaustive but these are validated instruments.
Stigma can also be perpetrated at the macro level through structural stigma by society through its laws, policies, organizational norms, and physical infrastructure. Structural stigma can disadvantage people with epilepsy limiting their opportunities and resources. Healthcare is fraught with examples of structural stigma.9
How can we address the stigma surrounding epilepsy?
Watch the full video to learn more about the stigma experienced by individuals with Epilepsy as well as how we can address the stigma surrounding Epilepsy.
Risk Factors
Risk factors for experiencing stigma
A 2022 International League against Epilepsy (ILAE) systematic review identified several risk factors for experiencing epilepsy-associated stigma, including higher seizure frequency, younger age at seizure onset, longer duration of epilepsy, lower educational levels, and poor epilepsy-specific knowledge.10 In the African setting where untreated seizures often result in visible scars, particularly burn scars, epilepsy stigmata are also associated with more felt stigma.11 This simplified view of stigma omits consideration of the reality that people live in complex situations in which they can have more than one health condition that is associated with stigma. For example, someone who has cerebral palsy and epilepsy might also have mobility constraints that subject them to stigma. Furthermore, beyond health-related stigma, there are other aspects of an individual than can subject them to stigma such as belonging to an ethnic minority or being poor. Intersectional stigma arises when multiple marginalized identities converge.12 Stigma burden also flows along power gradients such that individuals who are less powerful socially, economically, etc. are likely to be differentially burdened. For example, when given identical clinical case vignettes of a person living with epilepsy that differed only by gender and wealth, Zambian traditional healers attributed epilepsy in a poor woman as being a punishment for bad behavior while in a wealthy man epilepsy was ascribed to someone jealous bewitching the man.
For example, someone who has cerebral palsy and epilepsy might also have mobility constraints that subject them to stigma. Furthermore, beyond health-related stigma, there are other aspects of an individual than can subject them to stigma such as belonging to an ethnic minority or being poor.
Risk factors for stigmatizing
In studies of the general population, individuals who are older and less educated are more likely to stigmatize people with epilepsy.10 Interestingly, even the use of the term “epilepsy” instead of something more descriptive, such as ‘seizure disorder’ may be a contributor to stigmatizing attitudes among the general public.10 In Zambia, we undertook a series of stigma surveys among groups we identified as entities that hold some significant role in the lives of people with epilepsy. These included healthcare workers, teachers, clerics, and police officers. Using Knowledge, Attitude, Belief, and Practice Surveys, we found different predictors of stigmatizing attitudes within each group. Among healthcare workers, self-perceived competency to care for epilepsy was a strong predictor of stigmatizing suggesting that simply improving epilepsy care training may reduce epilepsy-associated stigma emanating from healthcare professionals.13 For clerics, most of whom had very limited education, stigmatizing attitudes were driven by whether or not the cleric understood epilepsy to be a medical condition rather than a spiritual problem.5 Among the police, stigmatizing attitudes and practices were associated with contagion beliefs such that persons with epilepsy, particularly those with a public seizure, were thought to represent a threat to public health.14 Finally, among teachers, almost all of whom understood the medical nature of epilepsy, less stigmatizing attitudes and practices were reported among those who had some person proximity to a person with epilepsy who was not a relative.15
Consequences
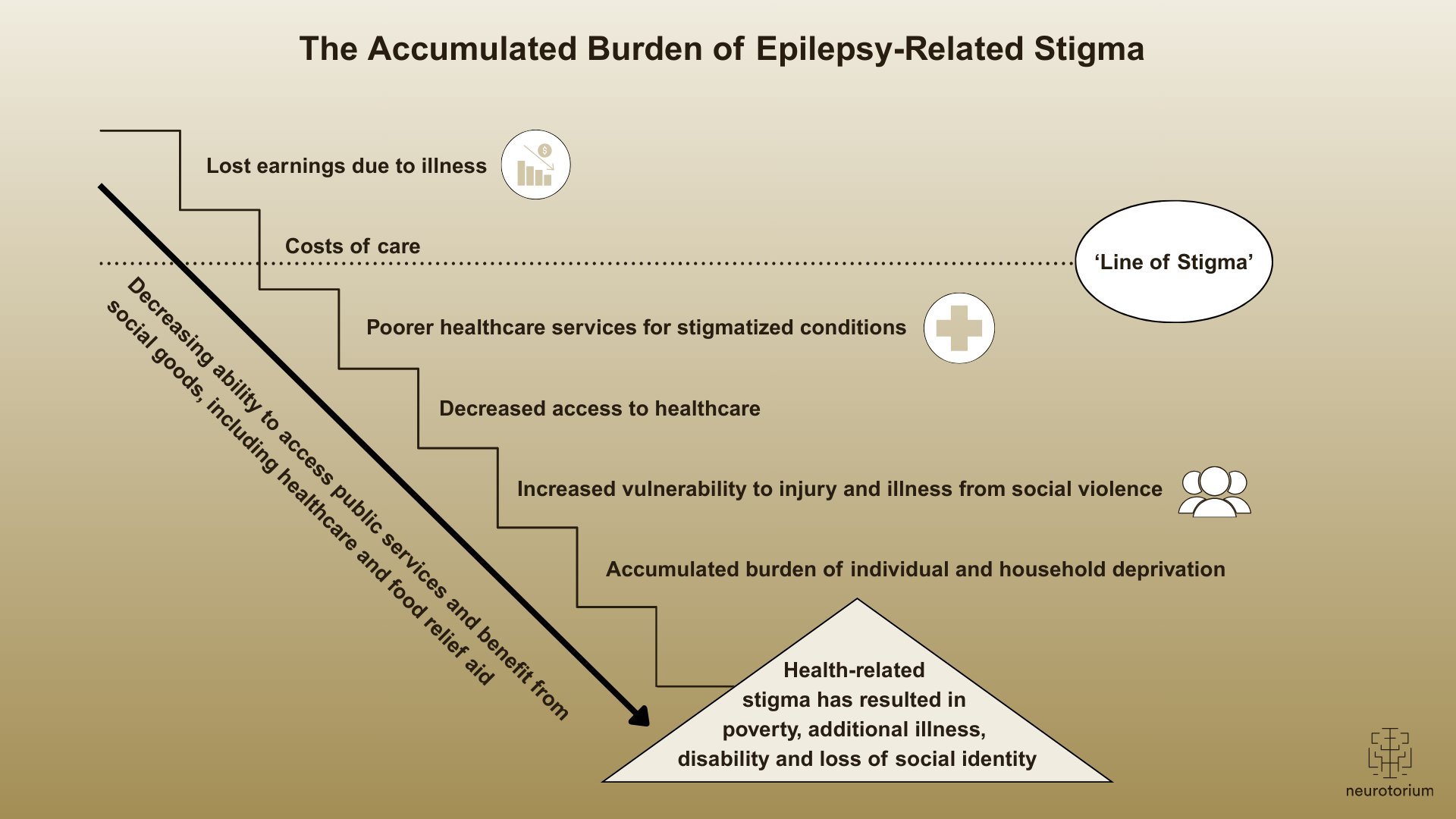
In the United Kingdom and Europe, epilepsy-associated stigma is associated with negative self-perceptions, anxiety, depression, poor quality of life, social isolation, and lower socioeconomic status.16-18 In less developed regions, epilepsy associated stigma is associated with less education, poorer socioeconomic status, being unmarried or separated, anxiety, and depression, including severe manifestations involving suicidal ideation.19 However, these analyses are confounded by being cross-sectional reports. Is someone poor because they are stigmatized, or stigmatized because they have epilepsy and are also poor? This analytic approach also fails to capture the complexity of co-occurring individual and structural stigmas. Figure 1 considers the potential accumulated social, economic, and medical burden of epilepsy-associated stigma.
Is someone poor because they are stigmatized, or stigmatized because they have epilepsy and are also poor?
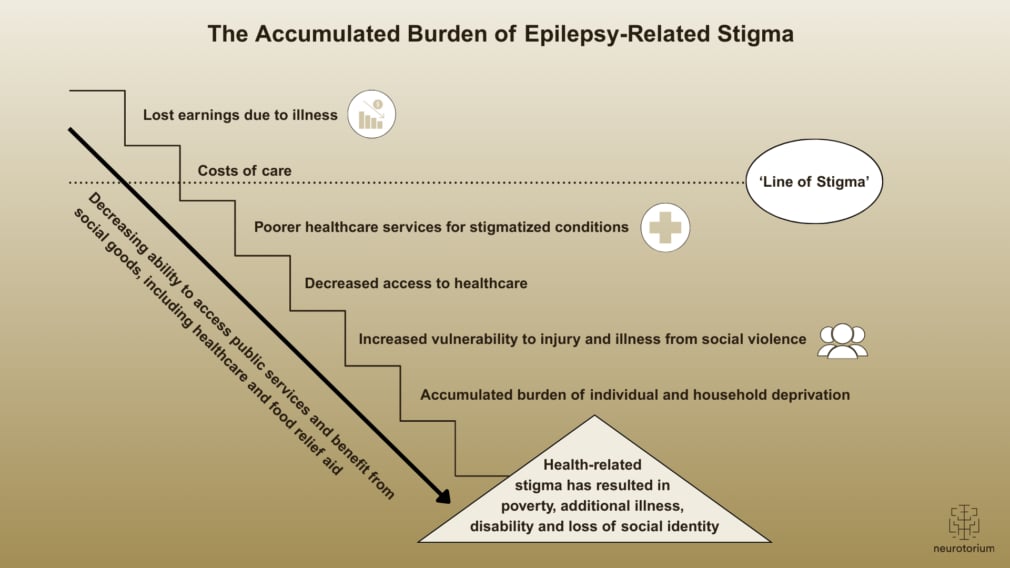
Figure 1: The accumulated burden of epilepsy-related stigma
The macro and micro level aspects of epilepsy-associated stigma may impact on all aspects of a person’s life, and the burden is cumulative. This figure provides an overview of some of these factors and the destructive, cumulative burden they place on the PWE medically, socially, and economically.
Stigma Reduction Interventions
Despite the great need, very few intervention studies aimed at stigma reduction in epilepsy have been undertaken and most of these are of poor quality.4 The ILAE first launched the “Out of the shadows” campaign in 199720 and early stigma reduction efforts were through mass social marketing campaigns, which are neither effective nor sustainable. The social constructs that contribute to health-related stigma and its structural barriers transcend any one condition. The best hope for meaningful, sustainable stigma reduction interventions in epilepsy may be collaborative efforts with stakeholders across a range of stigmatized conditions to develop, implement and evaluate interventions that can potentially improve the social and medical environments for multiple, marginalized conditions and identities.21
The social constructs that contribute to health-related stigma and its structural barriers transcend any one condition.
Related content
In this video, Professor Dr. Nathalie Jetté reviews depression as a common yet often under-recognized comorbidity in epilepsy.
In this video, Professor Dr. Gretchen Birbeck examines epilepsy-associated stigma as a global public-health challenge
{kind=link}
In this video, Professor Dr. Jacqueline French reviews practical, first-line decision-making for anti-seizure medication selection