Slide Decks on Epilepsy
According to the International League Against Epilepsy (ILAE), an epileptic seizure is “a transient occurrence of signs and/or symptoms due to abnormal, excessive, or synchronous neuronal activity in the brain”. The definition of epilepsy requires the occurrence of at least one epileptic seizure.
Epilepsy affects over 50 million people globally, with nearly 80% of people with epilepsy living in low- and lower-middle-income countries. Causes are diverse – ranging from genetic and structural factors to infection, inflammation, or stroke – yet many cases remain unexplained.
Epilepsy can affect daily functioning, health, and quality of life in many ways. For many individuals living with epilepsy, social stigma adds a layer of burden beyond the seizures themselves. The goal of epilepsy treatment is to eliminate seizures with no to minimal side effects or safety concerns. Some individuals may develop drug-resistant epilepsy, which may be defined as “the persistence of seizures despite at least two syndrome-adapted anti-seizure medications used at an efficacious daily dose”.
Understanding epilepsies’ biological, clinical, and social dimensions is essential for improving care and outcomes for people living with epilepsy. Each slide deck below introduces central topics and fundamental concepts related to epilepsy, all developed by leading experts in the field. All our slide decks are entirely free to download and use.
Interested in understanding seizure triggers and prevention?
History, Definitions, and Diagnosis
This slide deck introduces the history of epilepsy as a long-recognized disorder, definitions of seizures, classifications of epilepsies, as well as status epilepticus.
Epidemiology and Burden
This slide deck introduces both the epidemiology and burden of epilepsy, including stigma and quality of life, while acknowledging the barriers to accurate estimation of epilepsy burden.
Course, Natural History, and Prognosis
This slide deck provides an overview of the course and prognosis of epilepsy, from the risk of seizure recurrence after a first unprovoked seizure to the course of treated epilepsy.
Neurobiology and Aetiology
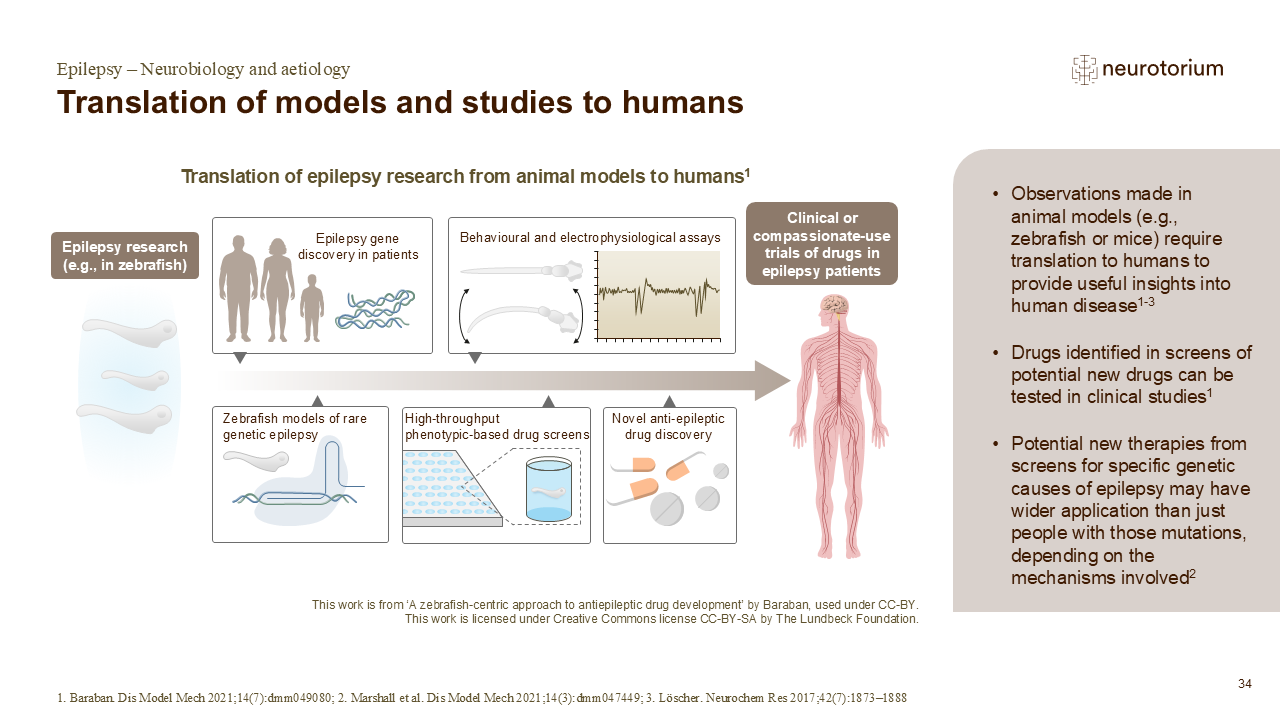
This slide deck provides an overview of the neurobiology and aetiology of epilepsy, exploring how various factors, including genetics, structural and metabolic causes, and inflammation, contribute to the disorder.
Comorbidities
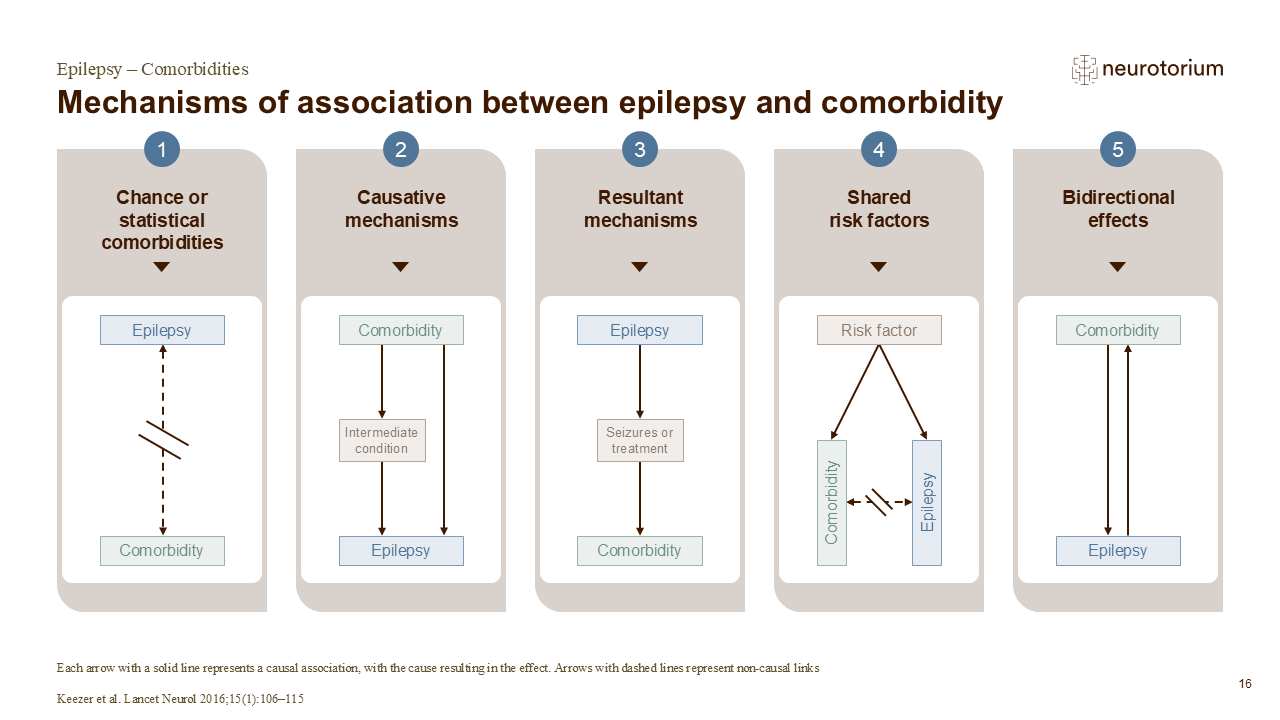
This slide deck explores the wide range of comorbidities associated with epilepsy and highlights their significant impact on the quality of life of persons living with epilepsy. The many mechanisms of comorbidity are also discussed.

Treatment Principles
This slide deck covers the principles of epilepsy treatment and strategies for initial and long-term care, including personalizing treatment and non-pharmacological interventions.
Articles about Epilepsy
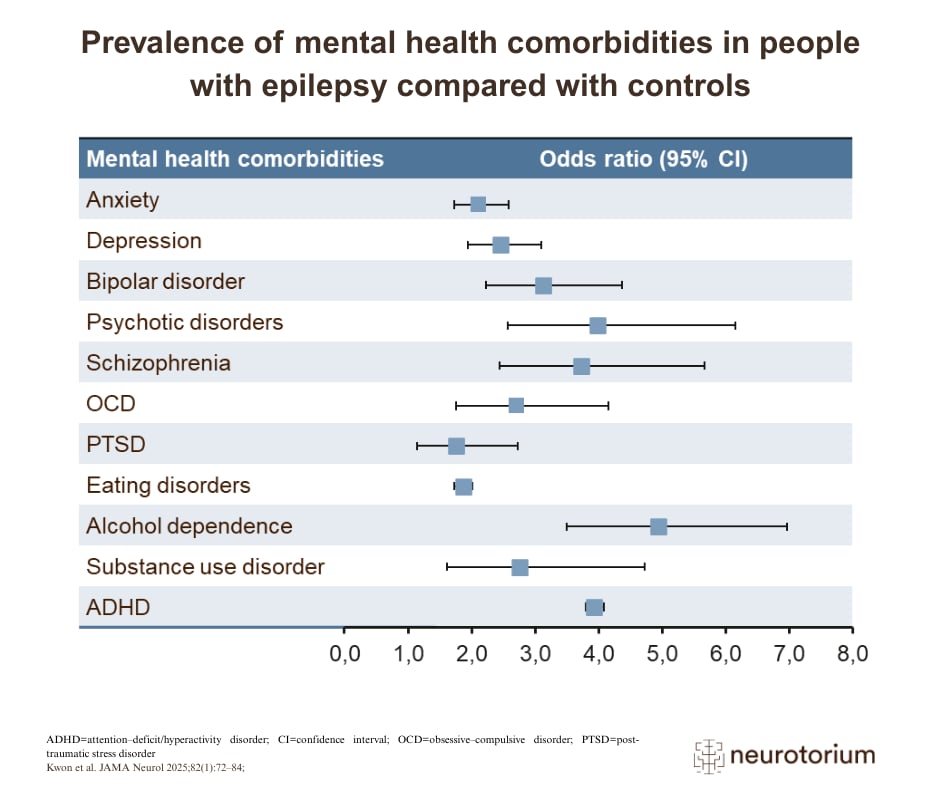
The complexity of epilepsy extends far beyond seizures, affecting health, daily functioning, and overall quality of life. Due to the stigma and medical and social disability associated with epilepsy, people with epilepsy are socially disadvantaged, with a lower quality of life relative to their peers. Also, psychiatric comorbidity is common in people with epilepsy, who are up to 8 times more likely than the general population to experience depression, anxiety, bipolar disorder, ADHD, sleep disorders, and other neuropsychiatric conditions.
The following articles highlight essential topics surrounding epilepsy and its clinical practice, including psychiatric comorbidities and the impact of stigma on people living with epilepsy.
- Psychiatric Comorbidities in Epilepsy
 Psychiatric comorbidities such as depression, anxiety and psychosis are highly prevalent in persons with epilepsy, profoundly influencing quality of life, seizure outcomes, and mortality.
Psychiatric comorbidities such as depression, anxiety and psychosis are highly prevalent in persons with epilepsy, profoundly influencing quality of life, seizure outcomes, and mortality. - Epilepsy-Associated Stigma: The Burden Beyond Seizures
 Fear, rejection, and “othering” of people living with epilepsy continues to be a major additional burden, a burden beyond seizures, for many people globally.
Fear, rejection, and “othering” of people living with epilepsy continues to be a major additional burden, a burden beyond seizures, for many people globally.
Watch Videos about Epilepsy
Explore our epilepsy video series, where leading experts break down complex topics and discuss key challenges in clinical care. Learn more about stigma, comorbidities, treatment considerations, global disparities in care, as well as emerging advances in disease-modifying therapies.

Stigma surrounding epilepsy
In this video, Professor Dr. Gretchen Birbeck examines epilepsy-associated stigma as a global public-health challenge.

Epilepsy in low- and middle-income countries
In this video, Professor Dr. Ley Sander discusses the challenges in delivering epilepsy care in low- and middle-income countries.

Depression comorbidity in epilepsy
In this video, Professor Dr. Nathalie Jetté reviews depression as a common yet often under-recognized comorbidity in epilepsy.
Disease-modifying therapies for acquired epilepsies
In this video, Professor Dr. Amy Brooks-Kayal outlines the field’s shift from seizure control to true disease modification in epilepsy.

The initial selection of an anti-seizure medication
In this video, Professor Dr. Jacqueline French reviews practical, first-line decision-making for anti-seizure medication selection.

Challenges in the clinical care of underserved populations
Professors Gabriele Fischer and Gretchen Birbeck discuss the impact of stigma on vulnerable populations with psychiatric and neurological disorders, highlighting education, systemic change, and integrated care as solutions.
Illustrations & Figures on Epilepsy
You can download and use our free images illustrating key scientific and clinical concepts of epilepsy. Below is a selection; you can find more images via the button below.
Frequently Asked Questions (FAQ)
The information provided in this document is for educational purposes only and is not a substitute for medical care. If you have questions about your health, speak with a healthcare professional.
Epilepsy is a chronic neurological condition of the brain that affects individuals of all ages. It is one of the most common neurological disorders, estimated to affect more than 50 million people worldwide, the majority of whom live in low- and middle-income countries. Epilepsy is associated with a substantial burden of disease due to its medical, psychological, and social impacts.
Epilepsy is characterized by a persistent predisposition or susceptibility to experience seizures. A seizure is a transient episode of abnormal, excessive or synchronous electrical activity in the brain. Seizures can vary widely in how they appear and how long they last. Some are visible and involve loss of consciousness or shaking of the body, while others may not be easily observable, such as brief lapses in awareness or involuntary movements. However, in most individuals with epilepsy, seizures tend to follow a consistent, stereotyped pattern, typically consisting of one or two recurrent seizure types. In contrast, the presence of multiple different types of events within a single individual may suggest an alternative diagnosis, such as psychogenic nonepileptic events. Therefore, epilepsies can differ widely between individuals.
References
- Neurotorium. Epilepsy – History, Definitions, and Diagnosis. https://neurotorium.org/slidedeck/epilepsy-history-definitions-and-diagnosis/
- World Health Organization. Epilepsy: A Public Health Imperative. 171 https:// www.who.int/publications/i/item/epilepsy-a-public-health-imperative (2019).
- National Institute of Neurological Disorders and Stroke (NINDS). Epilepsy and Seizures | National Institute of Neurological Disorders and Stroke. https:// www.ninds.nih.gov/health-information/disorders/epilepsy-and-seizures.
- Epilepsy Society. What is epilepsy? https://epilepsysociety.org.uk/about- epilepsy/what-epilepsy (2024).
- Isik, K., Morkavuk, G., Mete, B. & Koc, G. Comparison of Semiologic Characteristics of Psychogenic Nonepileptic Seizures and Frontal and Temporal Lobe Seizures. Neurol. Sci. Neurophysiol. 39, 126–131 (2022)
Epilepsy can arise from a wide range of underlying causes. In some individuals, epilepsy has a genetic basis. Genetic changes may be inherited or may occur spontaneously. Genetic causes may also contribute to variation in epilepsy symptoms and severity between individuals.
Epilepsy may also result from structural changes in the brain. These can occur during brain development before birth, due to genetic or environmental factors, or later in life following events such as stroke, infection, or traumatic brain injury. Structural abnormalities may alter brain architecture, reduce cortical thickness, or damage regions predisposed to seizure generation. Additionally, a wide range of inherited metabolic conditions can affect pathways in the brain involved in energy metabolism, neurotransmitter function, or synaptic activity and cause epilepsy.
References
- Neurotorium. Epilepsy – Neurobiology and Aetiology. https://neurotorium.org/slidedeck/epilepsy-neurobiology-and-aetiology/
- McTague, A., Howell, K. B., Cross, J. H., Kurian, M. A. & Scheffer, I. E. The genetic landscape of the epileptic encephalopathies of infancy and childhood. Lancet Neurol. 15, 304–316 (2016).
- Leventer, R. J., Guerrini, R. & Dobyns, W. B. Malformations of cortical development and epilepsy. Dialogues Clin. Neurosci. 10, 47–62 (2008).
- Oegema, R. et al. International consensus recommendations on the diagnostic work-up for malformations of cortical development. Nat. Rev. Neurol. 16, 618– 635 (2020).
- Pease, M. et al. Risk Factors and Incidence of Epilepsy after Severe Traumatic Brain Injury. Ann. Neurol. 92, 663–669 (2022).
- Fordington, S. & Manford, M. A review of seizures and epilepsy following traumatic brain injury. J. Neurol. 267, 3105–3111 (2020).
- Rho, J. M. & Boison, D. The metabolic basis of epilepsy. Nat. Rev. Neurol. 18, 333–347 (2022).
- Tumiene, B., Ferreira, C. R. & van Karnebeek, C. D. M. 2022 Overview of Metabolic Epilepsies. Genes 13, 508 (2022).
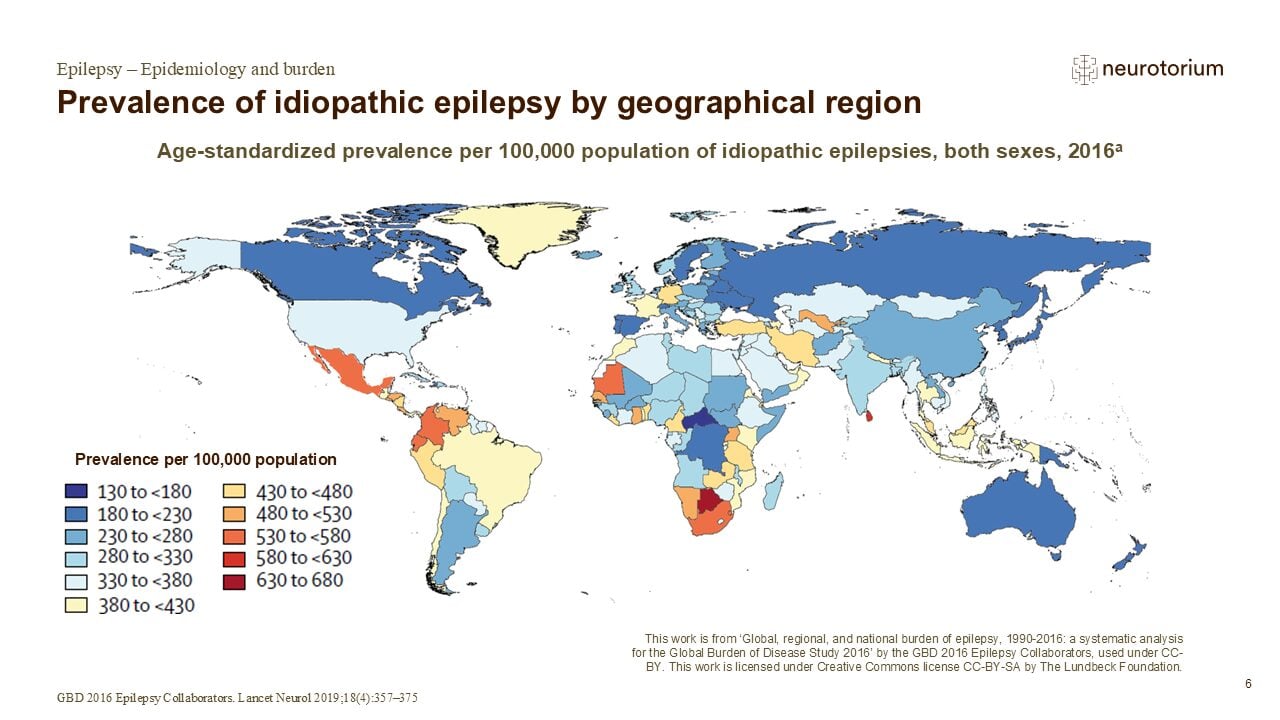
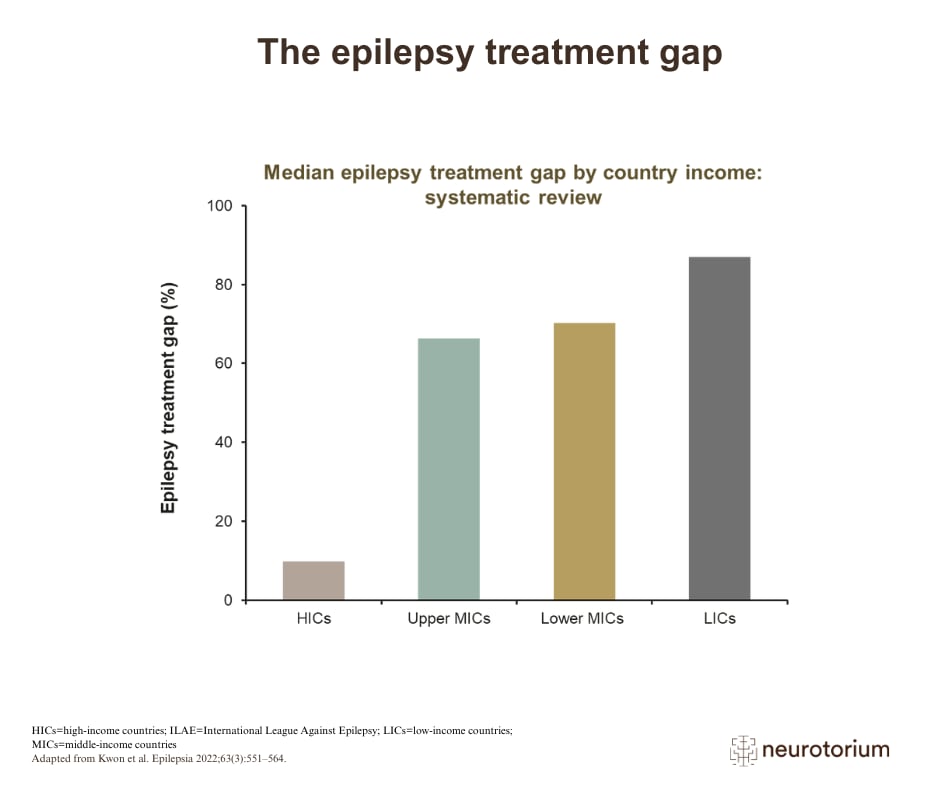
Epilepsy is estimated to affect around 50 million people globally, accounting for >0.5% of the global burden of disease according to the World Health Organisation (WHO). Highest prevalences have been observed in eastern, western, and southern sub- Saharan Africa, central Asia, Andean Latin America, and southeast Asia, with approximately 80% of persons with epilepsy living in low- and middleincome countries. This uneven global distribution might be caused by factors such as higher exposure to infections and brain injuries, suboptimal perinatal care, and limited access to timely diagnosis and treatment.
The true number of people living with epilepsy is likely underestimated. In many regions, epilepsy is under-recognized and under-diagnosed due to limited healthcare resources, lack of trained healthcare professionals, restricted access to diagnostic tools, and financial or geographic barriers to care seeking. Social stigma, fear of disclosure, and misunderstanding of symptoms also contribute to people not seeking or receiving appropriate medical attention.
References
- Neurotorium. Epilepsy – Epidemiology and Burden. https://neurotorium.org/slidedeck/epilepsy-epidemiology-and-burden/
- World Health Organization. Epilepsy: A Public Health Imperative. 171 https:// www.who.int/publications/i/item/epilepsy-a-public-health-imperative (2019).
- Beghi, E. et al. Global, regional, and national burden of epilepsy, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 18, 357–375 (2019).
- Beghi, E. & Hesdorffer, D. Prevalence of epilepsy–an unknown quantity. Epilepsia 55, 963–967 (2014).
- Pellinen, J. Treatment gaps in epilepsy. Front. Epidemiol. 2, 976039 (2022).
- Nicholas, A. Unlocking the hidden burden of epilepsy in Africa: Understanding the challenges and harnessing opportunities for improved care. Health Sci. Rep. 6, e1220 (2023).
The most recognizable symptom of epilepsy is recurrent seizures, but the experience of epilepsy is not the same for everyone.
Seizures occur when there is a sudden burst of abnormal electrical activity in the brain. Depending on which areas of the brain are involved, seizures may be very different. Some seizures are brief or invisible or not easy to detect, such as momentary lapses in awareness, staring spells, or small, involuntary movements. Sometimes the person having brief seizures is not even aware they are occurring. Other seizures are more obvious and may involve loss of consciousness, stiffening of the body, or sudden falls. Seizures can last from a few seconds to several minutes.
Beyond seizures, some people with epilepsy experience additional symptoms or difficulties. These can include difficulties with concentration or memory, changes in mood, anxiety or depression, sleep disturbances, or increased fatigue. Such symptoms may be related to seizure activity, underlying brain changes, antiseizure medications or the broader impact of living with a long-term neurological condition.
References
- Neurotorium. Epilepsy – Course, Natural History, and Prognosis. https://neurotorium.org/slidedeck/epilepsy-course-natural-history-and-prognosis/
- National Health System, UK. Epilepsy. nhs.uk https://www.nhs.uk/conditions/ epilepsy/ (2025).
- Shlobin, N. A. & Sander, J. W. Learning from the comorbidities of epilepsy. Curr. Opin. Neurol. 35, 175–180 (2022).
Epilepsy is diagnosed based on a combination of clinical history and supportive medical tests, rather than a single definitive test.
Because seizures may be brief and unpredictable, diagnosis relies heavily on reports from the individual and, when possible, from eyewitnesses who observed the event. Details such as changes in awareness, movements, duration, and triggers can provide crucial information.
Medical tests are used to support the clinical diagnosis and to better understand the underlying brain activity; however, imaging studies and electroencephalograms (EEGs) may be entirely normal in many individuals with epilepsy. Diagnostic tools such as neurophysiology, neuroimaging, neuropathology, and genetic testing can be helpful in guiding therapy and understanding the cause and prognosis, but they are not required to establish the diagnosis.
References
- Neurotorium. Epilepsy – History, Definitions, and Diagnosis. https://neurotorium.org/slidedeck/epilepsy-history-definitions-and-diagnosis/
- National Institute of Neurological Disorders and Stroke (NINDS). Epilepsy and Seizures | National Institute of Neurological Disorders and Stroke. https:// www.ninds.nih.gov/health-information/disorders/epilepsy-and-seizures.
- International League Against Epilepsy. The 2014 Definition of Epilepsy: A perspective for patients and caregivers. ilae.org https://www.ilae.org/ guidelines/definition-and-classification/the-2014-definition-of-epilepsy-a- perspective-for-patients-and-caregivers (2014).
- ILAE. EpilepsyDiagnosis.org. https://www.epilepsydiagnosis.org/.
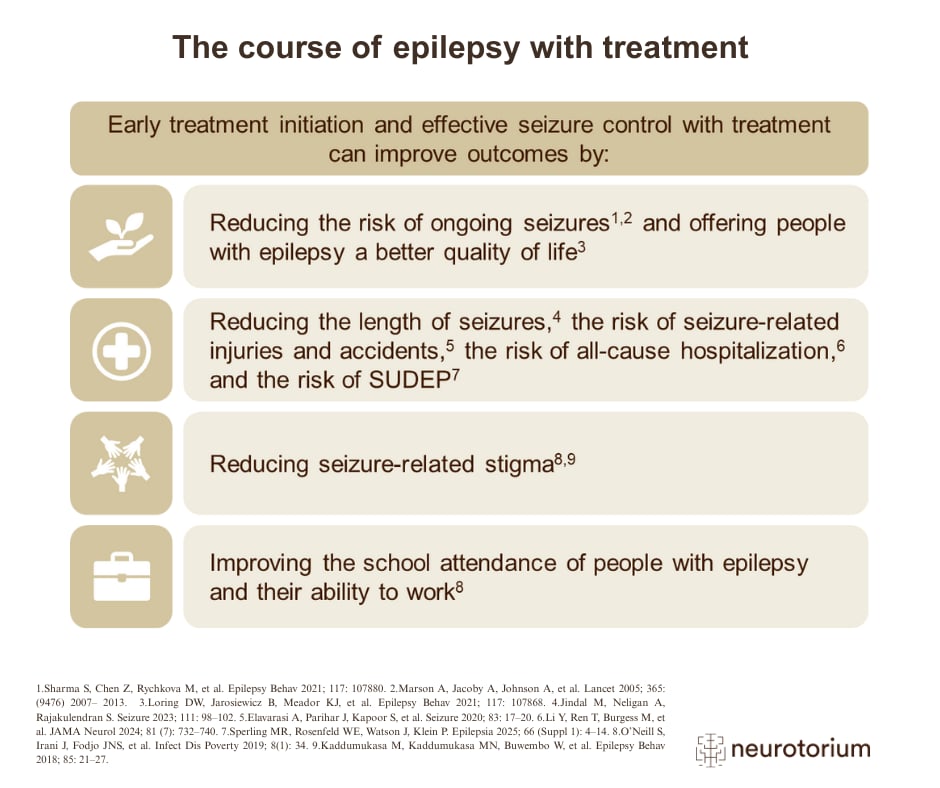
With appropriate use of antiseizure medications, the majority of individuals can live seizure-free. When complete seizure freedom cannot be achieved, treatment aims to reduce seizure frequency as much as possible while preserving quality of life and limiting treatment-related adverse effects.
For most people, treatment begins with a single antiseizure medication (ASM). The choice of medication is individualized and depends on several factors, including age, sex, pregnancy considerations, the type and cause of epilepsy, coexisting medical conditions, and potential interactions with other medications. Antiseizure medication is generally not required for provoked seizures if the provoking cause can be identified and eliminated.
If seizures are not adequately controlled with initial therapy, alternative medications or combination treatments may be considered. Some individuals may develop drug-resistant epilepsy, which is defined as the failure of adequate trials of two appropriately chosen and tolerated ASMs. In such cases, additional treatment options such as surgery or other techniques may be explored. Non-pharmacological interventions may be effective for selected individuals with drug-resistant epilepsy.
References
- Neurotorium. Epilepsy – Treatment Principles. https://neurotorium.org/slidedeck/epilepsy-treatment-principles/
- Friedman, D. Surgical Treatments, Devices, and Nonmedical Management of Epilepsy. Contin. Minneap. Minn 31, 165–186 (2025).
- Kanner, A. M. & Bicchi, M. M. Antiseizure Medications for Adults With Epilepsy: A Review. JAMA 327, 1269–1281 (2022).
- Löscher, W. & Klein, P. The Pharmacology and Clinical Efficacy of Antiseizure Medications: From Bromide Salts to Cenobamate and Beyond. CNS Drugs 35, 935–963 (2021).
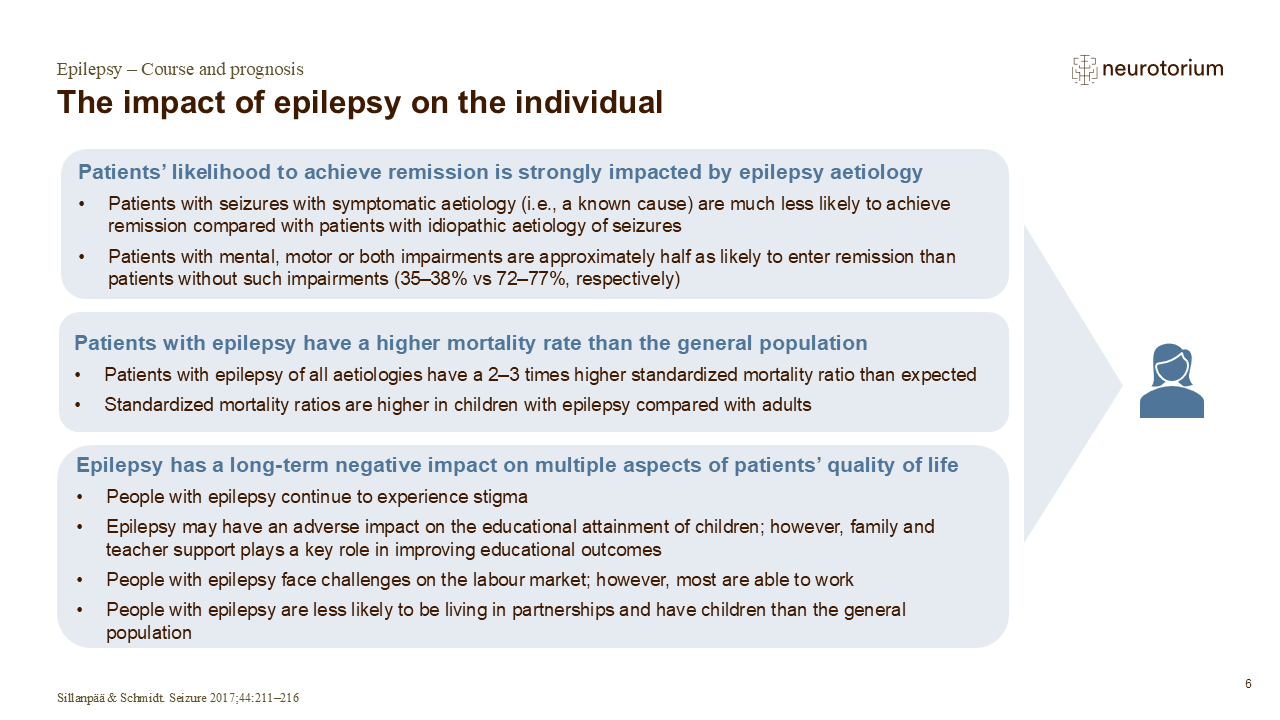
The problems experienced by persons with epilepsy are increasingly recognized as extending beyond just recurrent seizures. In addition to seizures, epilepsy can involve, psychological, and social consequences that significantly influence quality of life.
Research shows that people with epilepsy often experience a lower quality of life compared to their peers, not only because of seizures but also due to stigma, discrimination, and social exclusion. Misunderstanding of epilepsy and fear of seizures can contribute to marginalisation in education, employment, and social participation, further reducing well-being.
Supporting quality of life requires attention to both medical and social factors. Access to appropriate healthcare and recognition of co-existing conditions such as anxiety or depression are important, alongside social determinants, including education, employment, family support, and community inclusion which are critical. Evidence suggests that people with epilepsy are more likely to experience better outcomes when they have strong social support and meaningful employment, highlighting the importance of inclusive and supportive environments.
References
- Neurotorium. Epilepsy – Epidemiology and Burden. https://neurotorium.org/slidedeck/epilepsy-epidemiology-and-burden/
- World Health Organization. Epilepsy: A Public Health Imperative. 171 https:// www.who.int/publications/i/item/epilepsy-a-public-health-imperative (2019).
- Siebenbrodt, K. et al. Determinants of quality of life in adults with epilepsy: a multicenter, cross-sectional study from Germany. Neurol. Res. Pract. 5, 41 (2023).
- Mlinar, S., Petek, D., Coti č , Ž., Mencin Č eplak, M. & Zaletel, M. Persons with Epilepsy: Between Social Inclusion and Marginalisation. Behav. Neurol. 2016, 2018509 (2016).
- Obiako, O. R. et al. Factors affecting epilepsy treatment outcomes in Nigeria. Acta Neurol. Scand. 130, 360–367 (2014).
- ASM (antiseizure medication): Medications used to prevent or manage seizures in individuals with epilepsy.
- Cortical thickness: A measure of the thickness of the brain’s outer layer (the cortex), which is involved in functions such as thinking, perception, and decision-making. Most seizures originate from cortical areas.
- ILAE (International League Against Epilepsy): A global organization dedicated to advancing research, education, and care in the field of epilepsy.
- Metabolic conditions: Disorders that affect the body’s ability to convert food into energy or maintain bodily functions.
- Neurophysiology: The study of how the brain and nervous system function, including how nerve cells communicate and regulate behavior and bodily processes.
- Neuroimaging: Techniques used to visualize the structure or activity of the brain to support understanding of normal function and disease.
- Neuropathology: The study of diseases affecting the brain and nervous system through examination of structural and cellular changes in tissue.
- Non-pharmacological interventions: Healthcare interventions that do not primarily rely on medication; in epilepsy, examples include surgery, vagus nerve stimulation, and ketogenic dietary therapy.
- Perinatal care: Medical and supportive care provided to the mother and infant during pregnancy, childbirth, and the early postnatal period.
- Social stigma: Negative labelling and social disapproval of individuals or groups based on a perceived difference or trait, often leading to exclusion, discrimination, or loss of social status.
- Triggers: Factors that increase the likelihood of a seizure occurring in some individuals, such as stress, lack of sleep, alcohol consumption, or missed medication.
References
- World Health Organization. Epilepsy: A Public Health Imperative. 171 https:// www.who.int/publications/i/item/epilepsy-a-public-health-imperative (2019).
- National Institute of Neurological Disorders and Stroke (NINDS). Epilepsy and Seizures | National Institute of Neurological Disorders and Stroke. https:// www.ninds.nih.gov/health-information/disorders/epilepsy-and-seizures.
- International League Against Epilepsy. The 2014 Definition of Epilepsy: A perspective for patients and caregivers. ilae.org https://www.ilae.org/ guidelines/definition-and-classification/the-2014-definition-of-epilepsy-a- perspective-for-patients-and-caregivers (2014).
- ILAE. EpilepsyDiagnosis.org. https://www.epilepsydiagnosis.org/.
- Friedman, D. Surgical Treatments, Devices, and Nonmedical Management of Epilepsy. Contin. Minneap. Minn 31, 165–186 (2025).
- Neuropathology – an overview | ScienceDirect Topics. https://www. sciencedirect.com/topics/medicine-and-dentistry/neuropathology.
- Neuroimaging – an overview | ScienceDirect Topics. https://www. sciencedirect.com/topics/psychology/neuroimaging.
- Neurophysiology – an overview | ScienceDirect Topics. https://www.sciencedirect.com/topics/neuroscience/neurophysiology.
- Metabolic Disorder – an overview | ScienceDirect Topics. https://www. sciencedirect.com/topics/pharmacology-toxicology-and-pharmaceutical-science/ metabolic-disorder
3D Brain Atlas
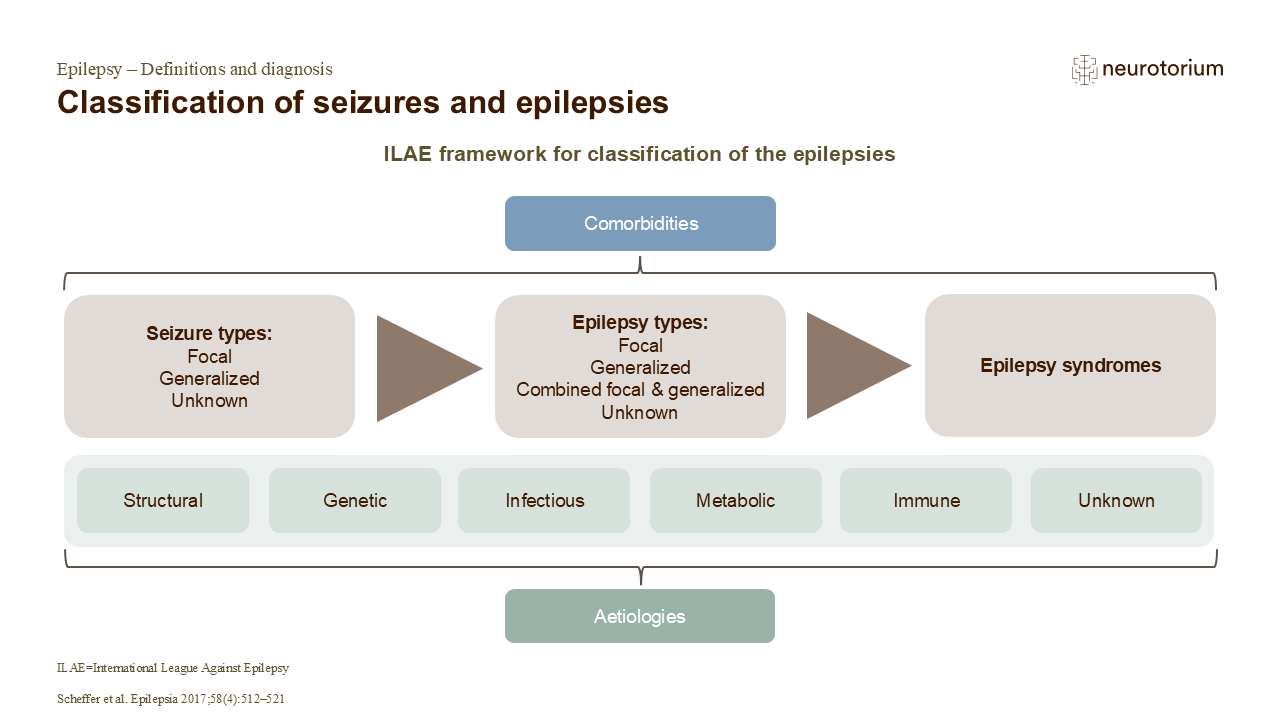
During seizures, neurons become hyperexcitable, and there is decreased inhibitory GABA signalling. With a focal seizure, the abnormal activity starts in one or more localized region(s) of the brain or hemisphere. With a generalized seizure, the abnormal activity starts across both hemispheres of the brain.
Neuroimaging and neuropathological studies have identified several structural and functional brain patterns associated with epilepsy. MRI analyses have shown altered subcortical volumes and reduced cortical grey-matter thickness. People with mesial temporal lobe epilepsies with hippocampal sclerosis specifically showed reduced volume in part of the hippocampus, and lower thickness in extrahippocampal cortical regions.
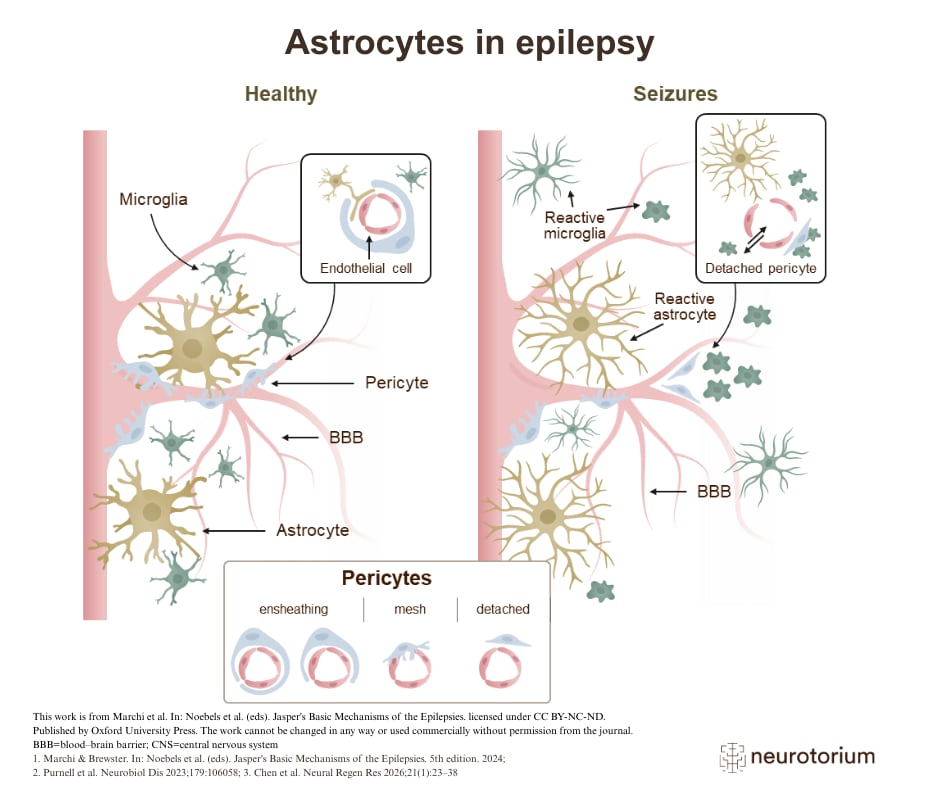
Also, a seizure is an inflammatory event, which can itself induce neuroinflammation. Chronic inflammation of the brain comprises:
– Activation of microglia, astrocytes, and peripheral immune cells
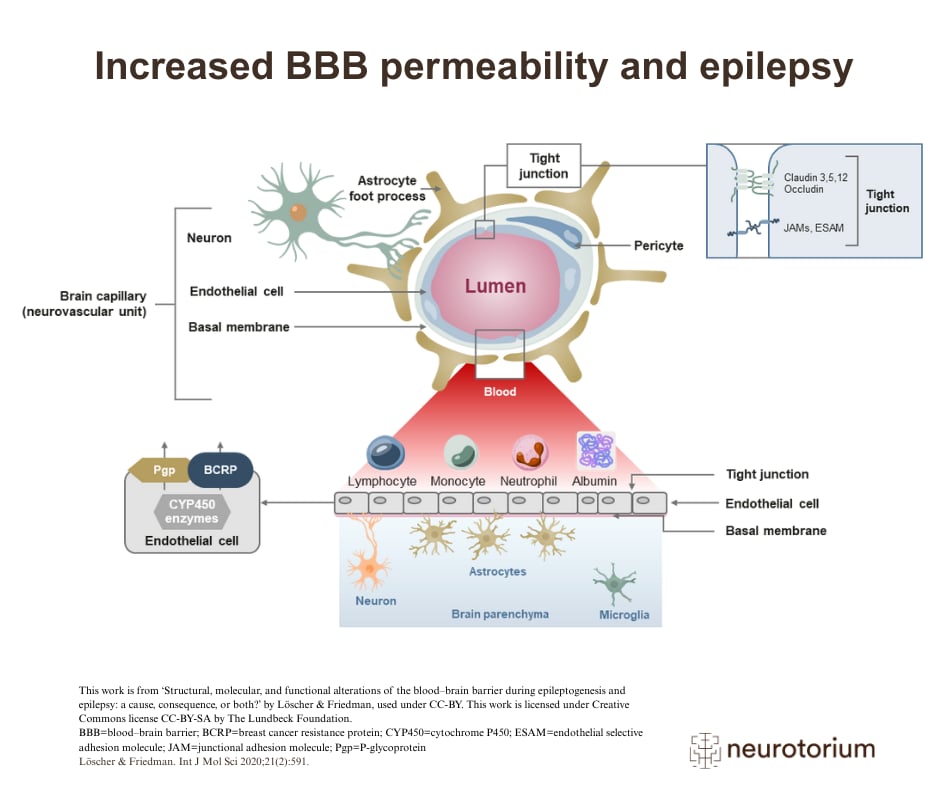
– Activation of the endothelial cells of the blood–brain barrier
– Production of inflammatory mediators
Inflammation is viewed by some as an intrinsic part of some forms of epilepsy, being the cause of, as well as the result of, a seizure. More research is needed to understand the role of inflammation in epileptogenesis and to confirm observations from preclinical studies.1