

Introduction
Epilepsy is one of the most common chronic neurological disorders, affecting more than 50 million people worldwide.1 Although seizures define the condition, epilepsy is much more than a disorder of recurrent seizures. Psychiatric comorbidities are highly prevalent among persons with epilepsy (PWE). Depression, anxiety, psychosis, and suicidality all occur at significantly higher rates in people with epilepsy compared to the general population, and yet they remain underrecognized and undertreated.2
For many patients, psychiatric symptoms are more distressing than seizures. Depression, in particular, is consistently associated with poorer health-related quality of life, reduced adherence to medication, and increased risk of premature death.3 The consequences extend beyond the clinic: people with epilepsy who experience psychiatric comorbidities may be less likely to complete education, secure employment, or form stable social relationships. The burden is not limited to high-income countries; indeed, in low- and middle-income countries (LMICs), stigma and health system limitations magnify the impact of psychiatric comorbidity.
Although seizures define the condition, epilepsy is much more than a disorder of recurrent seizures.
Psychiatric comorbidity in people with epilepsy
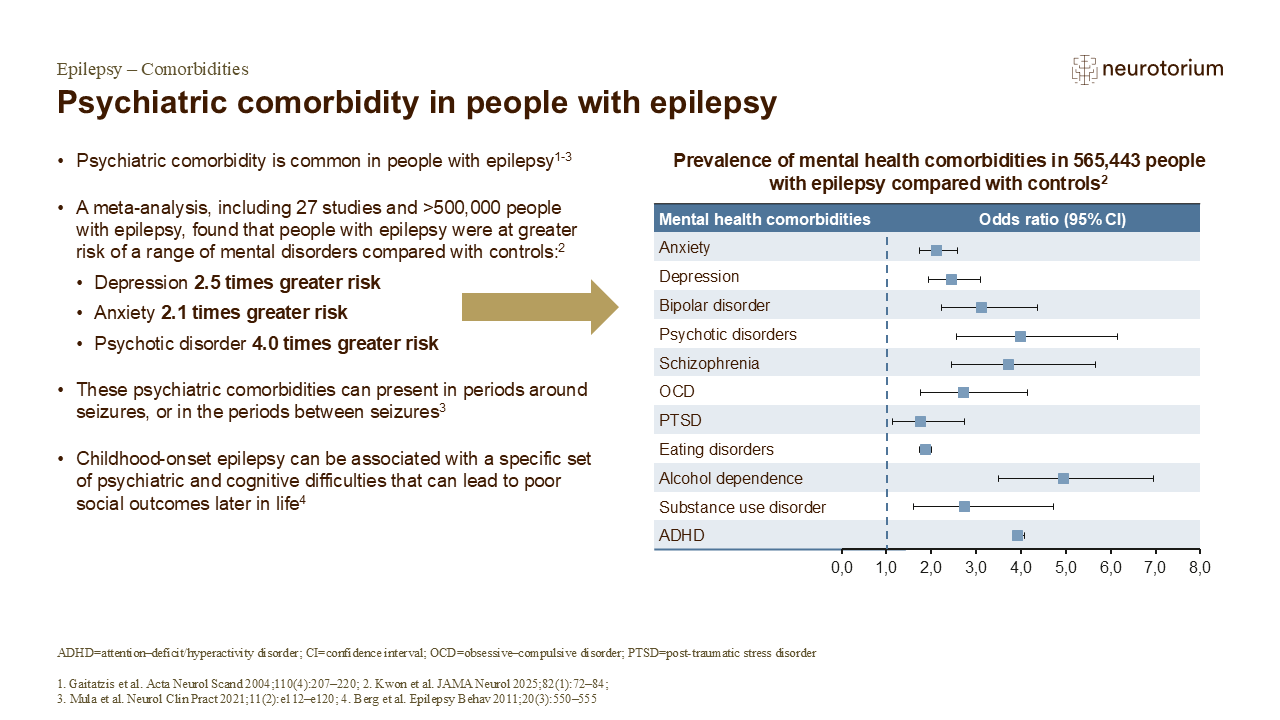
Given the significant impact of psychiatric comorbidities on patients’ overall morbidity burden and their general quality of life, appropriate identification and treatment of any psychiatric comorbidities in people with epilepsy is crucial for effective treatment.2 Moreover, in the meta-analysis by Kwon et al. summarized on the slide, the authors were careful to emphasize that many patients with epilepsy will have multiple comorbid psychiatric disorders, potentially putting them at risk for additional, more severe psychiatric complications, or other adverse outcomes (e.g., cognitive problems, suicidality).2,3 As such, routine screening for psychiatric comorbidities with reliable and validated tools is recommended by multiple epilepsy treatment guidelines,2 and people with epilepsy and any psychiatric comorbidity should receive a comprehensive individualized treatment plan, developed in cooperation with a multidisciplinary team of neurologists, psychiatrists, clinical psychologists and social workers to ensure the best treatment outcomes.3
References:
Epidemiology and Risk Factors
Epidemiological studies consistently show that up to half of individuals with epilepsy will experience a psychiatric disorder over their lifetime.4 Depression is the most common, with prevalence estimates of 20-30%, while anxiety disorders affect around 20%.5,6 Psychotic disorders, though less frequent, occur in 2-7% of patients, representing a several-fold increase compared to the general population.7 Suicide risk is particularly concerning: individuals with epilepsy are three to five times more likely to die by suicide than those without epilepsy.8 Functional/dissociative seizures (also known as psychogenic nonepileptic seizures) are another major psychiatric comorbidity encountered in epilepsy clinics. While not epileptic in origin, they frequently co-occur with epilepsy and share many risk factors, including early-life trauma, psychiatric comorbidities, and psychosocial stressors. Prevalence estimates suggest that up to 10–20% of patients referred to epilepsy centers have functional seizures, with approximately 10–30% of these cases also having coexisting epilepsy.9
Depression is the most common, with prevalence estimates of 20-30%, while anxiety disorders affect around 20%.5,6
Recent systematic reviews and meta-analyses provide the most comprehensive evidence to date. Persons with epilepsy have significantly higher rates of depression, anxiety, psychosis, bipolar disorder, and suicidality compared with people without epilepsy, across diverse populations worldwide.2 Importantly, these associations persist even after adjusting for confounding medical and social factors. Complementary evidence has also highlighted multipsychiatric comorbidity, showing that people with epilepsy are substantially more likely than controls to experience more than one psychiatric disorder concurrently.10 This underscores that psychiatric burden in epilepsy is not only common but often complex, with overlapping syndromes that may require tailored, multidisciplinary care.
Not all patients are equally affected. Temporal lobe epilepsy (TLE) and other forms of drug-resistant epilepsy carry the highest psychiatric burden. Epilepsy onset in childhood or adolescence is also associated with elevated risk, reflecting the vulnerability of the developing brain and the psychosocial impact of growing up with seizures. Several modifiable and non-modifiable risk factors contribute. Adverse effects of antiseizure medications (ASMs), polytherapy, and drug-drug interactions can provoke or worsen psychiatric symptoms.11 Genetic susceptibility also plays a role, with evidence that a family history of psychiatric illness increases risk.12 Social determinants of health, such as poverty, isolation, and discrimination, can further exacerbate vulnerability, particularly in LMICs where treatment gaps are largest.13
Importantly, these associations persist even after adjusting for confounding medical and social factors.
Pathophysiological Mechanisms
The strong association between epilepsy and psychiatric disorders is not coincidental. Shared neurobiological pathways link the two. Limbic circuits, including the hippocampus and amygdala, play central roles in both seizure generation and emotional regulation.14 Alterations in prefrontal cortical function and connectivity in large-scale brain networks, such as the default mode and salience networks, contribute to impaired cognition and affect. Interictal epileptiform activity and structural lesions may further disrupt these systems, contributing to psychiatric vulnerability.15 Evidence also supports a bidirectional relationship where psychiatric disorders can precede epilepsy onset. A history of depression, for example, is associated with increased risk of developing epilepsy, suggesting shared etiological mechanisms rather than simple causation.16 Pharmacological influences add complexity. While lamotrigine can improve both mood and seizure control, ASMs such as levetiracetam or topiramate may provoke irritability, anxiety, or depression in some patients.17 Recognizing medication-related effects is critical for treatment planning. Finally, systemic processes such as hypothalamic-pituitary-adrenal (HPA) axis dysregulation, chronic stress, and neuroinflammation contribute to both seizure susceptibility and psychiatric morbidity.18
Limbic circuits, including the hippocampus and amygdala, play central roles in both seizure generation and emotional regulation.14
Mechanisms of association between epilepsy and comorbidity
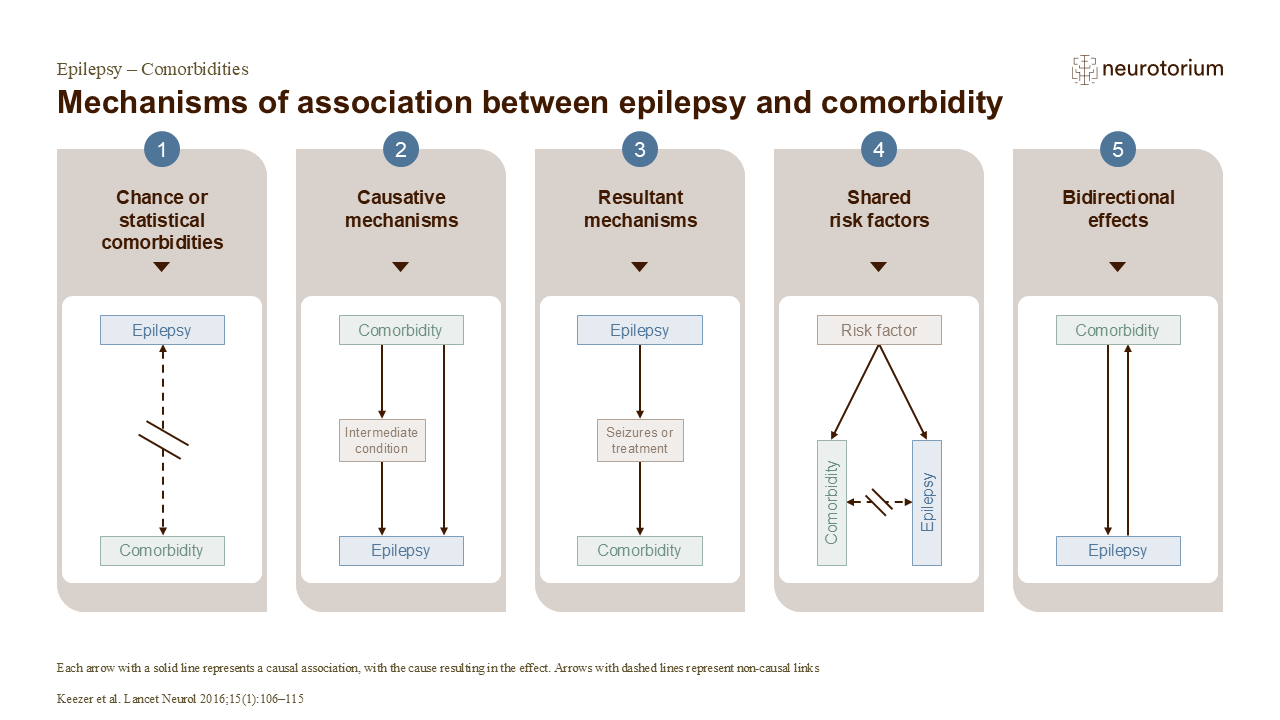
Chance comorbidities are conditions that are as frequent in people with epilepsy as would be expected in the general population; in statistical comorbidities, non-causal associations between epilepsy and a comorbid condition arise as a result of information or selection bias rather than a true causal link.1
In a causative association between a comorbidity and epilepsy, comorbidity appears first and then gives rise to epilepsy directly (e.g., cerebrovascular disease) or indirectly (e.g., cigarette smoking can indirectly cause epilepsy by increasing the risk of cancer or stroke).1 In a resultant association between epilepsy and a comorbidity, the temporal link is reversed: for example, epilepsy may lead to aspiration pneumonia or seizure-related fractures.1
Moreover, epilepsy and other comorbid conditions may not have a direct association with each other, but they may share genetic, environmental, structural or physiological risk factors.1
Finally, the relationship between epilepsy and certain comorbidities may be bidirectional, i.e., either condition can cause the other; however, it is crucial to distinguish between truly bidirectional causality and varying temporal sequence of epilepsy and its comorbidities between different people.1
Reference:
Clinical Presentation and Diagnostic Challenges
Psychiatric comorbidities in epilepsy often present atypically, making diagnosis difficult. Fatigue, irritability, and cognitive slowing may reflect seizure burden, ASM side effects, or underlying psychiatric illness. Postictal psychosis may resemble primary psychotic disorders but typically emerges after seizure clusters and remits spontaneously.19 Anxiety can take the form of anticipatory fear of seizures or seizure-related panic attacks, further complicating differentiation from primary anxiety disorders. Functional seizures can further complicate diagnosis, as they may closely mimic epileptic events yet are psychologically mediated. Careful video-EEG monitoring is essential for accurate differentiation. Misdiagnosis may delay appropriate psychiatric treatment and expose patients to unnecessary ASM.20,21
Many individuals with epilepsy have multiple concurrent psychiatric diagnoses, often spanning mood, anxiety, and psychotic spectrums.10 This reality explains why diagnostic categories can appear blurred in clinical practice and why patients often fall through the cracks of siloed care systems. Cultural and systemic barriers compound these challenges. In many settings, patients may be reluctant to disclose psychiatric symptoms due to stigma or lack of trust. Health care providers may prioritize seizure control, neglecting psychological well-being. These dynamics are particularly pronounced in LMICs, where mental health literacy and specialist care remain limited. Validated screening tools can help. The Neurological Disorders Depression Inventory for Epilepsy (NDDI-E), the Generalized Anxiety Disorder 7-item scale (GAD-7), and the Patient Health Questionnaire (PHQ-9) are brief and practical instruments for use in clinical practice.22
Functional seizures can further complicate diagnosis, as they may closely mimic epileptic events yet are psychologically mediated.
Treatment and Management
Management of psychiatric comorbidities in epilepsy requires an integrated, multidisciplinary approach. Neurologists, psychiatrists, primary care providers, psychologists, and often social workers must collaborate to provide person-centered care.23
Pharmacological treatments are effective when used with attention to seizure thresholds and interactions. SSRIs are generally safe and effective for depression and anxiety in epilepsy, while medications such as bupropion and clozapine should be avoided or used with caution due to their proconvulsant potential.24 Some ASMs such as lamotrigine offer a dual benefit in controlling seizures and stabilizing mood.24
Psychological therapies play a vital role. Cognitive behavioral therapy (CBT) has been shown to reduce depressive symptoms in PWE, and acceptance and commitment therapy (ACT) has improved psychological flexibility and quality of life.25 Surgical approaches including resective epilepsy surgery and vagus nerve stimulation, may reduce both seizure frequency and psychiatric symptoms.26 Dietary therapies such as the ketogenic diet have shown some promise for mood improvement, though evidence remains limited.27 Given the markedly elevated suicide risk, routine suicide risk assessment should be part of every clinical encounter.8 Management of functional seizures requires a multidisciplinary approach, often centered on psychotherapeutic interventions such as CBT or trauma-focused therapy. Early recognition, empathetic communication of the diagnosis, and collaboration between neurology and psychiatry are critical to improving outcomes.28
Neurologists, psychiatrists, primary care providers, psychologists, and often social workers must collaborate to provide person-centered care.23
In this video, Professor Dr. Nathalie Jetté reviews depression as a common yet often under-recognized comorbidity in epilepsy. She notes that roughly one in three people with epilepsy meet criteria for depression at any given time, yet many are not screened in routine neurology care and a substantial proportion remain untreated. Practical assessment options are highlighted, such as structured/semi-structured interviews (MINI, SCID) and free tools such as the NDDI-E and PHQ-9. Understanding and treating depression in epilepsy is critically important, as it is linked to poorer response to anti-seizure medicines, more adverse effects, lower quality of life, and increased suicide risk.
Special Populations
Psychiatric comorbidities manifest differently across life stages and populations. Children and adolescents with epilepsy face higher rates of attention-deficit/hyperactivity disorder (ADHD), autism spectrum disorder (ASD), anxiety, and depression.29 Early recognition, family-centered interventions, and educational accommodations are essential to prevent long-term sequelae. In older adults, depression may mimic or exacerbate cognitive decline, leading to diagnostic uncertainty. Women with epilepsy experience increased rates of depression and anxiety, shaped by hormonal fluctuations, reproductive health issues, and gender-related social stressors. Mental health assessment should therefore be integrated into preconception counseling and perinatal care.30 Patients in LMICs face the most severe barriers. In many regions, the epilepsy treatment gap exceeds 75%, and psychiatric services are even less accessible.31 Community health worker models, task-shifting, and mobile health technologies are emerging strategies to bridge these gaps.
Future Directions
Recognition of psychiatric comorbidities as integral to epilepsy care marks an important paradigm shift. Several priorities are emerging. Routine screening and early intervention should be implemented across all care settings, using validated tools such as the NDDI-E. Integrated care models that bridge neurology and psychiatry are essential to overcome fragmentation of services. Research must continue to develop culturally tailored interventions to ensure global relevance and acceptability.
Emerging science offers additional promise. Biomarkers of inflammation, stress response, and neural network dysfunction may one day allow for earlier identification of patients at risk. Digital health tools, including smartphone-based mood tracking and seizure diaries, are increasingly feasible in both high- and low-resource settings. Implementation science will be critical to translating proven strategies into practice at scale, ensuring that evidence-based interventions reach those who need them most.
Conclusion
Psychiatric comorbidities are central, not peripheral, to epilepsy care. Depression, anxiety, psychosis, suicidality, and functional seizures profoundly affect quality of life, seizure control, and mortality. They complicate diagnosis, challenge treatment adherence, and drive stigma and social exclusion. Yet they are also modifiable, with effective screening tools, therapies, and models of care available. The future of epilepsy care must be interdisciplinary, culturally responsive, and globally minded. By addressing psychiatric comorbidities alongside seizures, clinicians can move beyond seizure control alone toward comprehensive, person-centered care that truly improves the lives of people with epilepsy.
Psychiatric comorbidities are central, not peripheral, to epilepsy care.
Related content
In this video, Professor Dr. Nathalie Jetté reviews depression as a common yet often under-recognized comorbidity in epilepsy.
In this video, Professor Dr. Gretchen Birbeck examines epilepsy-associated stigma as a global public-health challenge
In this video, Professor Dr. Jacqueline French reviews practical, first-line decision-making for anti-seizure medication selection