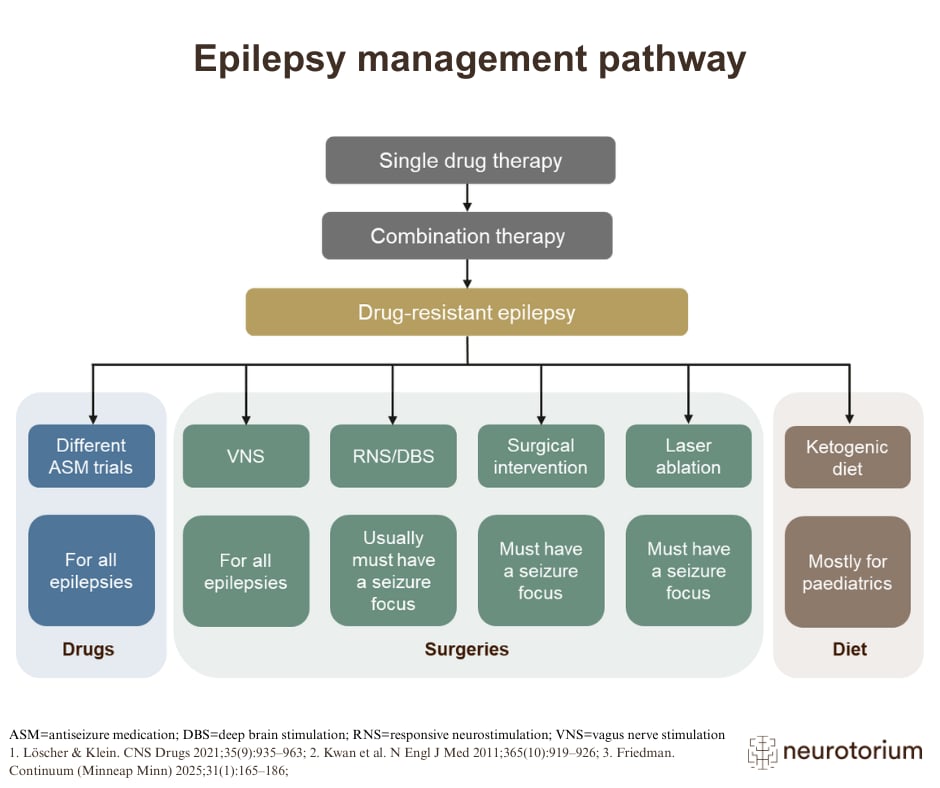
The image illustrates the current treatment paradigm for epilepsy. Monotherapy should be used for initial treatment4. However, if the initial therapy fails, either alternative monotherapy or adjunctive treatment (addition of a second drug to the first one) may be chosen; tolerability is a key consideration when making this decision1-4.
Risk‒benefit profile of any treatments should be carefully evaluated4. In addition, combinations that produce excessive adverse effects, or cause drug‒drug interactions should be avoided1-5.
ASM=antiseizure medication; DBS=deep brain stimulation; RNS=responsive neurostimulation; VNS=vagus nerve stimulation
Related content
In this video, Professor Dr. Nathalie Jetté reviews depression as a common yet often under-recognized comorbidity in epilepsy.
In this video, Professor Dr. Gretchen Birbeck examines epilepsy-associated stigma as a global public-health challenge
In this video, Professor Dr. Jacqueline French reviews practical, first-line decision-making for anti-seizure medication selection