


Introduction
Poor physical health and related disparities among people with mental disorders represent a global challenge across the full spectrum of mental disorders, reflecting both increased vulnerability to chronic physical diseases and reduced access to adequate healthcare.1 As a result, physical comorbidities are a major contributor to the markedly reduced life expectancy observed in people with mental disorders, while also amplifying personal, societal, and economic burden across the life course.1-3 The relationship between mental and physical health is bidirectional and self-reinforcing.2 Mental disorders increase the risk of developing physical illnesses and complicate their prevention and management, whereas the presence of physical comorbidity can hinder the treatment of mental disorder and restrict therapeutic options.2 When physical disease leads to fatigue, disability, or reduced mobility, it may further limit social participation, education, and employment, deepening social exclusion.1,2 In turn, these downstream effects can exacerbate mental health problems, creating a cycle in which mental and physical disorders mutually reinforce one another.1,2
The relationship between mental and physical health is bidirectional and self-reinforcing.2
Epidemiology of physical comorbidities in mental disorders
Worldwide, chronic physical diseases and mental disorders represent a growing and pressing health burden.4 Pooled estimates indicate that the coexistence of mental disorders and chronic physical diseases is particularly substantial in developing and emerging countries, where a recent meta-analysis reported a pooled prevalence of mental disorders of 36.6% among patients with chronic physical conditions and a pooled odds ratio of 3.1.4 The Lancet Psychiatry Commission identified nearly 100 systematic reviews and meta-analyses on physical comorbidities in mental disorders, most of which focused on cardiometabolic diseases and consistently showed a 1.4- to 2-fold higher risk of obesity, diabetes, and cardiovascular disease (CVD) compared with the general population.1 In severe mental illness (SMI), the pooled prevalence of CVD is estimated at 9.9%.5 In addition, depressive disorders, anxiety disorders, posttraumatic stress disorder, and sleep disorders are associated with an increased risk of acute coronary syndrome.6
Type 2 diabetes is among the most prevalent physical comorbidities, with pooled prevalence estimates ranging from 5% to 22% depending on the mental disorder.7-9 In inpatient psychiatric settings, pooled prevalence estimates are 10% for unspecified diabetes, 1% for type 1 diabetes, and 9% for type 2 diabetes.10 The pooled prevalence of metabolic syndrome in SMI is 32.6%, with antipsychotic-treated patients showing a higher risk of both diabetes and metabolic syndrome, but with some exceptions.8,11
Beyond cardiometabolic disease, respiratory diseases are also more common in certain mental disorders. Compared with the general population, people with schizophrenia have significantly higher rates of chronic obstructive pulmonary disease (COPD), asthma, and pneumonia, with a pooled prevalence of 7.7%, 7.5%, and 10.3%, respectively.12 Attention-deficit/hyperactivity disorders and bipolar disorders are also significantly associated with asthma, since childhood.13,14 Physical comorbidities are further amplified in SMI patients with co-occurring substance use disorders, particularly hypertension, tardive dyskinesia, and hepatitis C.15 The burden of infectious diseases may be underestimated, as it has been little studied beyond SMI.1 Available reviews in SMI populations report average incidences of 15.63% for hepatitis B, 7.21% for hepatitis C, 7.59% for HIV, and 1.1–7.6% for syphilis.1
In severe mental illness (SMI), the pooled prevalence of CVD is estimated at 9.9%.5

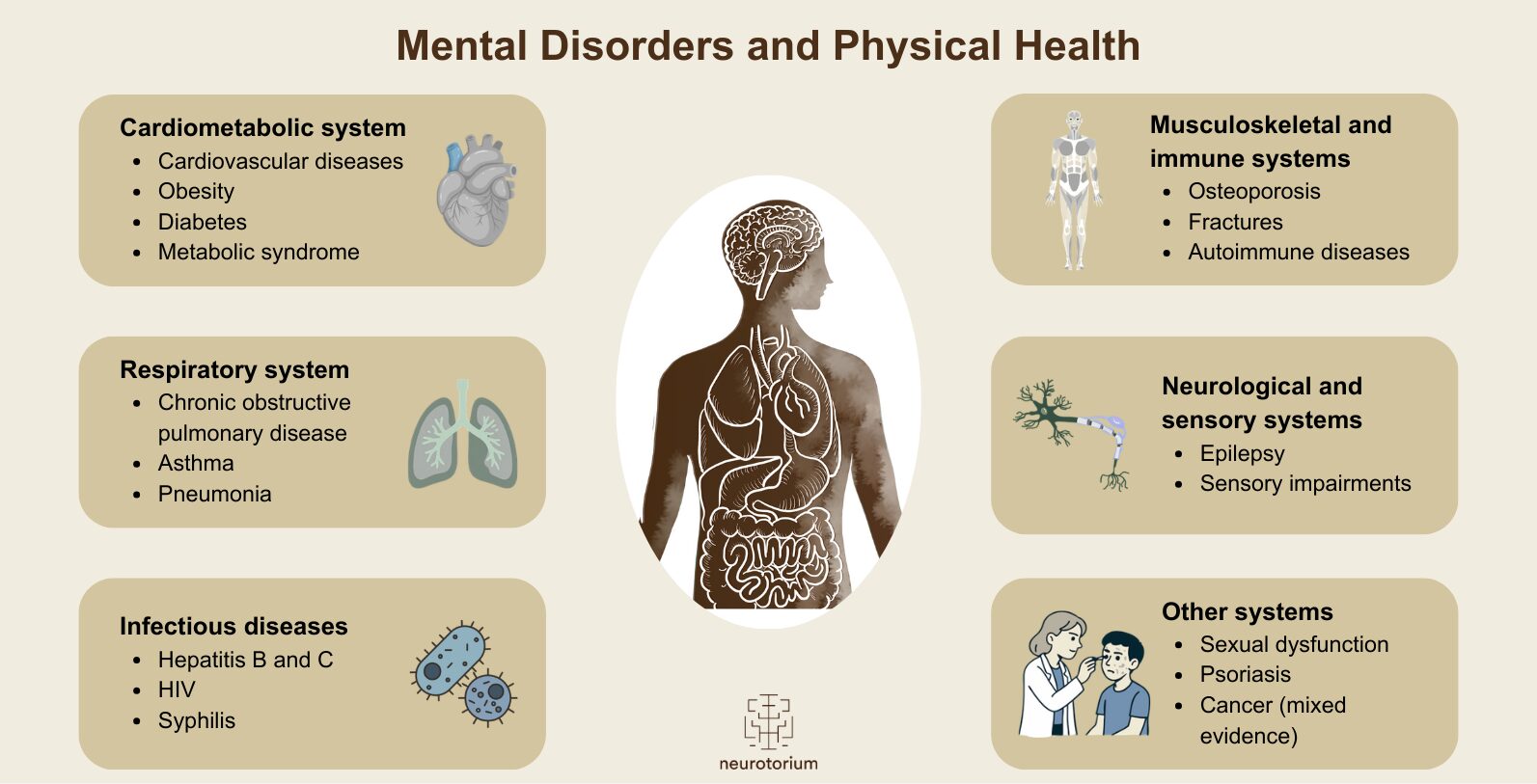
Figure 1. Main organ systems affected by physical comorbidities in people with mental disorders
Cardiometabolic conditions, including cardiovascular diseases, obesity, diabetes, and metabolic syndrome, represent the most consistently reported and prevalent comorbidities. Respiratory disorders are also more common, particularly in severe mental illness. Infectious diseases contribute substantially to morbidity, especially among individuals with co-occurring substance use disorders. Neurological and sensory conditions, musculoskeletal and immune-related disorders, and other conditions such as sexual dysfunction and psoriasis, further highlight the multisystem nature of physical illness in this population. Evidence linking mental disorders to cancer risk remains mixed. Many of these conditions co-occur within individuals, reflecting the high burden of physical multimorbidity across mental disorders.
A wide range of other physical conditions have also been linked to mental disorders, including sexual dysfunction, epilepsy, osteoporosis, fractures, psoriasis, autoimmune diseases, and sensory impairments.1,16-18 Evidence on cancer risk remains mixed, with reports ranging from slight increases to no association or reduced risk depending on cancer type.1 Figure 1 illustrates the main organ systems affected.
Importantly, two meta-analyses indicate that people with SMI are at substantially increased risk of physical multimorbidity, with odds ratios of 1.84 and 2.40 compared with those without SMI.19,20 Multimorbidity, defined as the coexistence of two or more chronic conditions, provides a broader and more patient-centered framework than traditional comorbidity.20 In one meta-analyses, the absolute prevalence of physical and psychiatric multimorbidity in people with SMI was found to be 25% and 14%, respectively, with particularly high vulnerability to physical multimorbidity at younger ages, likely reflecting the combined influence of early (e.g., prenatal, genetic, sociocultural factors) and later risk factors (e.g., choice of psychotropic drugs, lifestyle factors).20
Multimorbidity, defined as the coexistence of two or more chronic conditions, provides a broader and more patient-centered framework than traditional comorbidity.20
Mechanisms linking mental and physical health
The mechanisms linking mental disorders and physical diseases remain unclear but are likely multifactorial.21,22 Proposed explanations include direct interactions through physiological pathways such as the neuroendocrine system, bidirectional effects whereby physical conditions contribute to the development of mental disorders and mental disorders increase the risk of physical illness, as well as shared underlying risk factors including early-life trauma, chronic stress, inflammation, and socioeconomic disadvantage.22 Evidence further indicates that demographic, behavioral, lifestyle, and social factors, including older age, higher body mass index, female sex, smoking behavior, lower educational attainment, ethnicity, and childhood maltreatment, substantially shape the risk and pattern of non-communicable disease onset and physical multimorbidity among people with mental disorders.21,23 In addition, the physical health burden in this population may be compounded by the adverse effects of psychotropic medications and by systemic disparities in healthcare delivery, as individuals with mental disorders are less likely to receive adequate screening and high-quality treatment for conditions such as CVD, cancer, and diabetes.24-26
Proposed explanations include direct interactions through physiological pathways such as the neuroendocrine system, bidirectional effects whereby physical conditions contribute to the development of mental disorders and mental disorders increase the risk of physical illness, as well as shared underlying risk factors including early-life trauma, chronic stress, inflammation, and socioeconomic disadvantage.22
Impact of mental disorders on physical disease outcomes and resource use
People living with a chronic physical condition experience poorer clinical outcomes when a mental disorder is also present, including lower quality of life, heightened mortality risk, and reduced life expectancy relative to the general population, with 14.7 years of potential life lost (YPLL).21,27-37 Substance use disorders are linked to the greatest reduction in life expectancy, with an estimated 20 YPLL.28 Furthermore, people with SMI and co-occurring physical conditions face a higher risk of hospitalization than those with the physical condition alone, along with increased rates of readmission for certain conditions, including diabetes, CVD, and COPD.38 Physical comorbidities substantially increase healthcare use and costs for people with mental disorders, though impacts vary by care setting.39 Global estimates suggest over 30% excess use of inpatient, outpatient, and emergency care, and up to 45% higher costs in some sectors compared with those without physical comorbidities.39
Substance use disorders are linked to the greatest reduction in life expectancy, with an estimated 20 YPLL.28
Medication and treatments in general
The impact of treatments for mental disorders on physical health is more complex than would be expected from their adverse effect profiles alone.31,33,34,36, 40 For example, antipsychotics are well known to increase cardiometabolic risk, yet their use is associated with lower all-cause mortality compared with no treatment.33,34,36 This apparent “antipsychotic paradox” suggests that mortality in schizophrenia is shaped by multiple, interacting pathways rather than by single risk factors alone.40 Beyond symptom control, effective treatment may reduce stress-related biological dysregulation, support healthier behaviors, and maintain sustained engagement with healthcare services.33,40 Regular contact with mental health and primary care professionals facilitates monitoring, prevention, and earlier detection of physical disorders, potentially offsetting medication-related risks.33,40 In this way, effective psychiatric treatment may not only mitigate the mortality gap directly but also strengthen patients’ connection to health systems, improving both mental and physical health outcomes.31,33,40

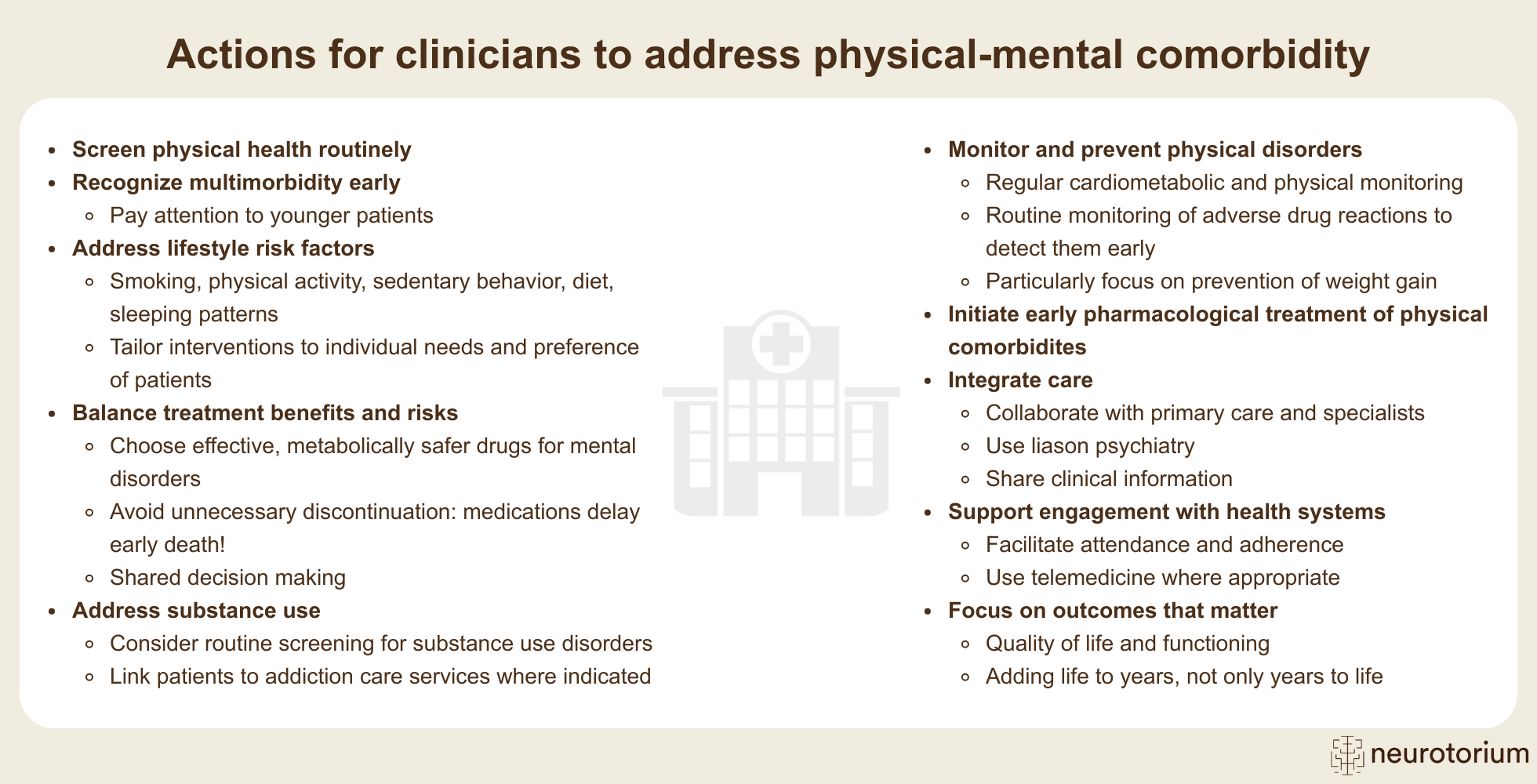
Figure 2. Key actions for clinicians to address physical–mental comorbidity
Key strategies include routine physical health screening, prevention and ongoing monitoring of physical disorders, addressing lifestyle risk factors and substance use, and ensuring early identification and treatment of physical comorbidities. It is also essential to balance treatment benefits and risks by selecting effective and metabolically safer treatments for mental disorders, avoiding unnecessary discontinuation, and engaging patients in shared decision-making. Integrated and collaborative care models, such as liaison psychiatry and close coordination with primary care and specialist services, support comprehensive and coordinated management. Collectively, these actions should aim to improve quality of life, functioning, and long-term health outcomes, adding life to years, not only years to life.
Clinical and public health implications
Mental–physical comorbidity represents a major global health equity challenge, as people with mental disorders continue to experience poorer access to quality healthcare.1 Addressing this gap requires a reorientation of mental health policies and services towards the simultaneous prevention, detection, and treatment of both mental and physical conditions.1,4 Integrated and collaborative care models, incorporating routine physical health screening within mental health services, are essential, especially in low- and middle-income settings where inequalities are greatest.4 Early intervention is critical given the higher burden of physical multimorbidity observed in younger individuals with SMI.20 Clinicians can further reduce avoidable mortality through ensuring patients receive early effective treatments including pharmacological and other biological treatments for mental and physical disorders, careful selection and monitoring of treatments, balancing effectiveness with adverse effects, and engaging patients in shared decision-making.40 Notably, effective treatment of mental disorders plays a central role in reducing excess mortality and delaying early death.31,34,36,40 Antipsychotic treatment in schizophrenia (long-acting injectable and clozapine in particular), as well as antidepressant use and electroconvulsive therapy in major depressive disorder, are consistently associated with lower all-cause mortality despite recognized treatment-related risks.31,34,36 Alongside pharmacological care, lifestyle interventions targeting smoking, physical inactivity, diet, and sleep should be embedded as core components of care, tailored to cognitive, motivational, and socio-economic needs.41 Together, these strategies aim not only to extend life expectancy but also to improve quality of life, functioning, and long-term wellbeing.40 Figure 2 summarizes key actions clinicians can take to address physical–mental comorbidity.
Early intervention is critical given the higher burden of physical multimorbidity observed in younger individuals with SMI.20
Future directions
Future research should prioritize longitudinal and life-course approaches to clarify the timing, accumulation, and trajectories of physical multimorbidity in people with mental disorders. Improved and standardized measurement of multimorbidity is needed to capture its complexity, severity, and dynamic nature across settings and populations. Conceptual frameworks that adopt systems-level perspectives may better reflect the interacting biological, behavioral, and social processes that drive co-occurring mental and physical illness. Although psychosocial and demographic risk factors for multimorbidity in SMI are increasingly recognized, the underlying mechanisms remain poorly understood.23 Greater emphasis on integrative mechanistic studies is required, including investigation of stress, inflammation, genetic and epigenetic processes, and neurobiological alterations, alongside social determinants of health. Advancing research across biological, psychological, and societal domains holds promise for identifying modifiable pathways and informing more effective prevention and intervention strategies.
Greater emphasis on integrative mechanistic studies is required, including investigation of stress, inflammation, genetic and epigenetic processes, and neurobiological alterations, alongside social determinants of health.
In this video, Professor Dr. Marco Solmi introduces what the mortality gap is and why there is a mortality gap in schizophrenia. He highlights both the individual-level lifestyle factors and system-level factors where people living with schizophrenia appear to receive poorer quality of care compared to people without schizophrenia. Dr. Solmi also explains what the antipsychotic paradox means and what healthcare professionals can do to help close this gap.
Conclusion
Physical health and mental disorders are closely linked, with mental–physical comorbidity posing a major global public health and equity challenge that drives excess morbidity, premature mortality, and healthcare costs. Addressing this burden requires coordinated, integrated, and equity-focused responses across clinical care, services, and policy, with emphasis on prevention, early detection, and effective pharmacological and non-pharmacological care across the life course.
Related content
Schizophrenia remains one of psychiatry’s most complex disorders due to its multifactorial etiology, involving interacting biological, psychological, and environmental factors.
{kind=link}
{kind=link}