

The Body- and Brain-First Model
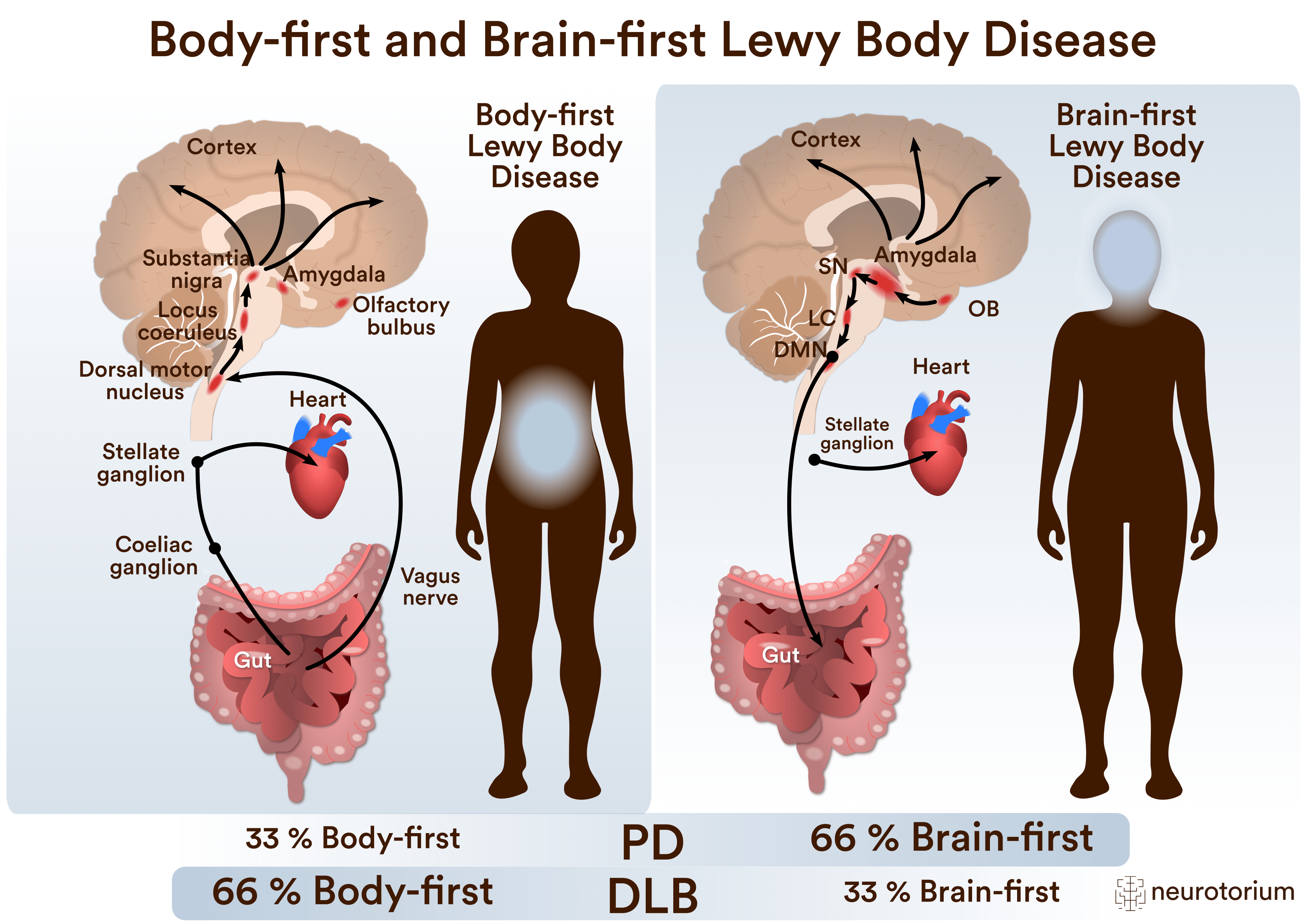
The BvB model proposes that in most cases of LBD, the first pathological alpha-synuclein aggregates are formed either in the gut or the olfactory bulb (Figure 1).4,10-13 In body-first LBD, Lewy pathology originates in the enteric nervous system of the gut and invades the brain via the parasympathetic vagus nerve and the sympathetic autonomic nerve fibres. These body-first patients commonly develop autonomic symptoms and REM sleep behaviour disorder (RBD) years before the clinical diagnosis. In contrast, most cases with brain-first LBD are triggered in the olfactory epithelium in the nose, where Lewy pathology invades the brain via the olfactory nerve. By this route, the pathology reaches the dopaminergic cells faster and the prodromal phase of brain-first LBD is therefore shorter. Brain-first patients generally do not develop autonomic problems or RBD before diagnosis – but most patients will develop these symptoms after diagnosis; however, most will develop these symptoms later as the spreading pathology inevitably affects all parts of the nervous system in advanced stages of LBD. Thus, while body- and brain-first patients start out very differently, they become increasingly similar as the disease progresses.
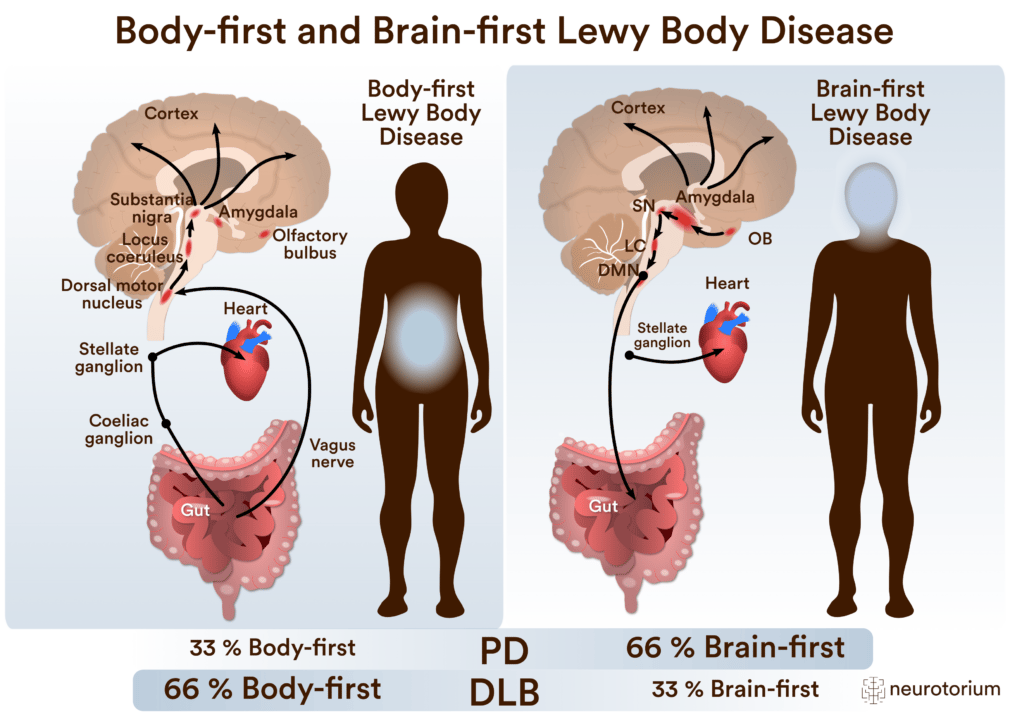
Figure 1: Body-First vs Brain-First Lewy Body Disease
Characteristics of proposed body-first and brain-first subtypes of Parkinson’s Disease (PD). Arrows indicate the direction of spread of α-synuclein pathology.
Clinical Brain- and Body-First Types
The clinical trajectory of LBD is often summarized as shown in Figure 2A. This creates the impression of a relatively homogeneous disease course, beginning with autonomic symptoms like constipation 20 years before diagnosis, followed by RBD and hyposmia, until finally motor symptoms emerge (Figure 2A). However, this disease trajectory is only representative of a minority of patients with Parkinson’s disease (PD) and is therefore an oversimplification.
In fact, only around one-third of PD patients develop RBD and constipation before diagnosis.14-16 The BvB model suggests that this clinical subtype reflects a body-first origin of the disease. The other two-thirds of PD patients typically do not develop RBD or constipation before parkinsonism emerges. Indeed, they have mild or sometimes no non-motor symptoms at the time of diagnoses (Figure 2B). The BvB model suggests that this clinical subtype with mild or no “bodily symptoms” before diagnosis reflects a brain-first origin of the disease, where the pathology is initiated in the olfactory system of the nose or sometimes in the brain itself (typically the limbic system).
Notably, most brain-first patients eventually develop the same symptoms as body-first patients, but in reversed order. Around one-third of PD patients have RBD at the time of diagnosis, and the sleep disorder typically appeared many years before motor symptoms. However, 10 years after diagnosis, 87% of PD patients have RBD, meaning that most of the originally RBD-negative patients have now developed RBD.17,18 The same trend is seen for constipation and many other symptoms.19
The BvB model posits that PD and dementia with Lewy bodies (DLB) are variants of the same disease. More specifically, that the Lewy pathology component in these two disease types is indistinguishable.20 On the other hand, it is well known that DLB patients on average have significantly more Alzheimer-type co-pathology compared to non-demented PD patients, which is believed to significantly contribute to the different clinical appearance of DLB.21,22
Importantly, the BvB model proposes that the majority of DLB patients have body-first Lewy body disease. Studies indicate that over two-thirds of DLB patients develop RBD before diagnosis.23-26 Other studies report that DLB patients develop much more frequent constipation, urinary dysfunction, and orthostatic hypotension prior to diagnosis when compared to PD.27 In summary, these findings suggest that most PD patients have brain-first Lewy body disease, whereas most DLB patients have body-first Lewy body disease.
In summary, these findings suggest that most PD patients have brain-first Lewy body disease, whereas most DLB patients have body-first Lewy body disease.

Figure 2: The Trajectory of Brain-First and Body-First PD
In Parkinson’s Disease (PD), the disease course is often summarized as depicted in panel A. Patients develop autonomic symptoms such as constipation and REM sleep behaviour disorder (RBD) 10-20 years before diagnosis. This trajectory is however only representative of around 1/3 of PD patients, but 2/3 or more of dementia with Lewy bodies patients follow this trajectory. B. The other 2/3 of PD patients typically follow the disease course depicted in panel B. They have mild or no obvious non-motor symptoms before diagnosis. Yet, most of these patients will develop RBD, autonomic problems and other symptoms after diagnosis.
Imaging Brain- and Body-First
If the BvB model is correct, it would be expected that imaging can demonstrate signs of neurodegeneration in the autonomic nervous system of the gut and heart years before dopamine loss commences in body-first patients. In contrast, brain-first patients should show signs of dopamine loss on brain scans first, and develop pathology on heart and gut imaging only later (Figure 3).
These studies require a complex set-up, as patients must undergo multiple imaging modalities, often unavailable within a single department. Also, patients need to be included at the earliest possible disease stage, where the contrasting brain- and body-first imaging patterns are clearest. As the disease progresses, LBD patients tend to converge and show pathology on most imaging parameters. It is also important to include other robust methodologies such as video-polysomnography to diagnose RBD, and to document whether RBD developed before or after diagnosis in the patient population.
Utilizing multi-modal imaging, it has been documented that approximately 95% of patients with isolated RBD (prodromal body-first LBD) exhibit severe degeneration of sympathetic terminals in the heart, measured by [123I]MIBG scans. In most RBD cases, the heart is invisible on these scans (Figure 3, top panel). In contrast, around 70% of these iRBD patients still have normal brain dopamine scans, and those patients with pathological dopamine scans generally show significantly less severe dopamine loss compared to newly diagnosed PD patients.13,28-31 Such iRBD patients also show delayed colonic transit time and enlarged colon volumes on CT scans compared to PD patients without RBD.32
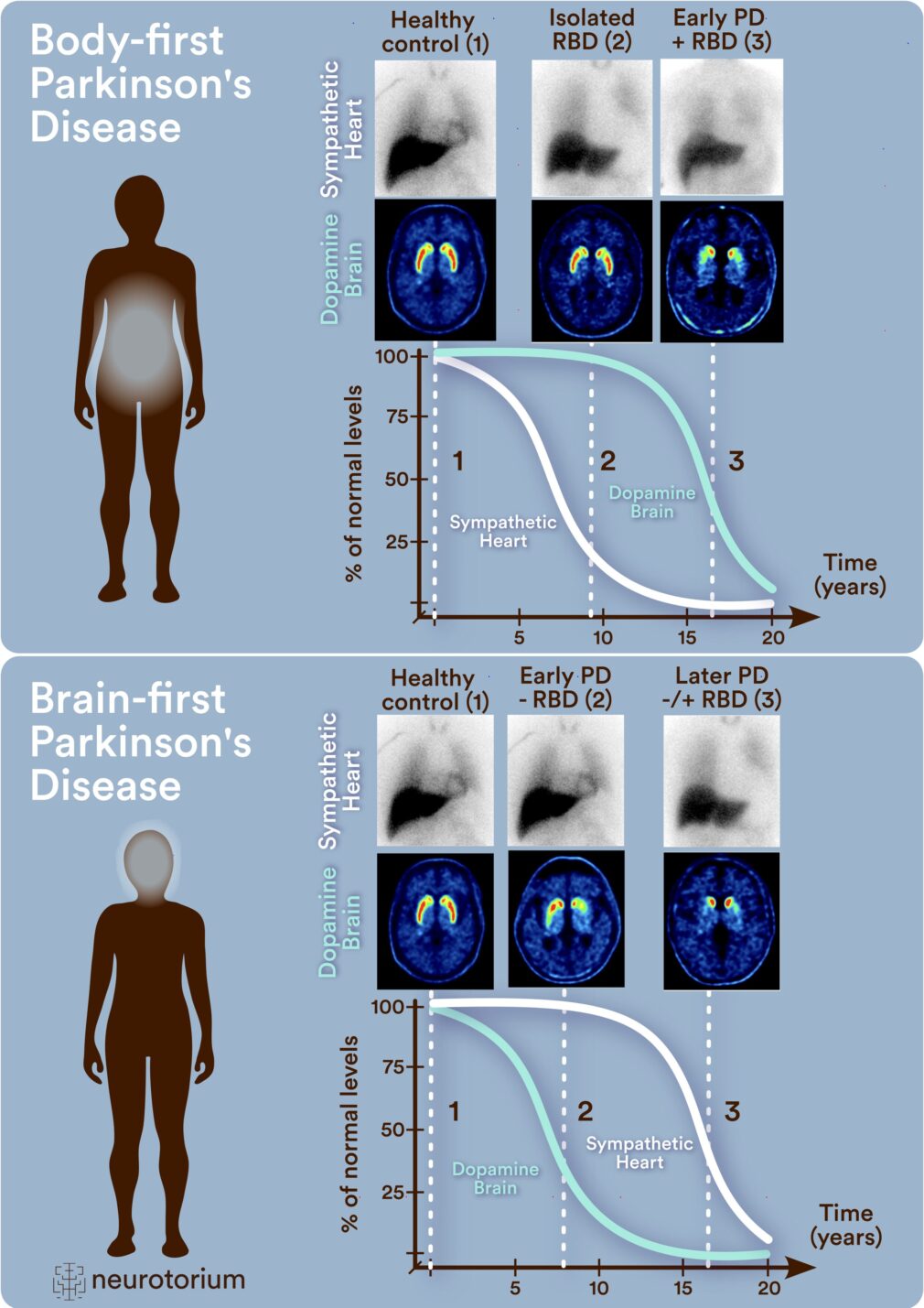
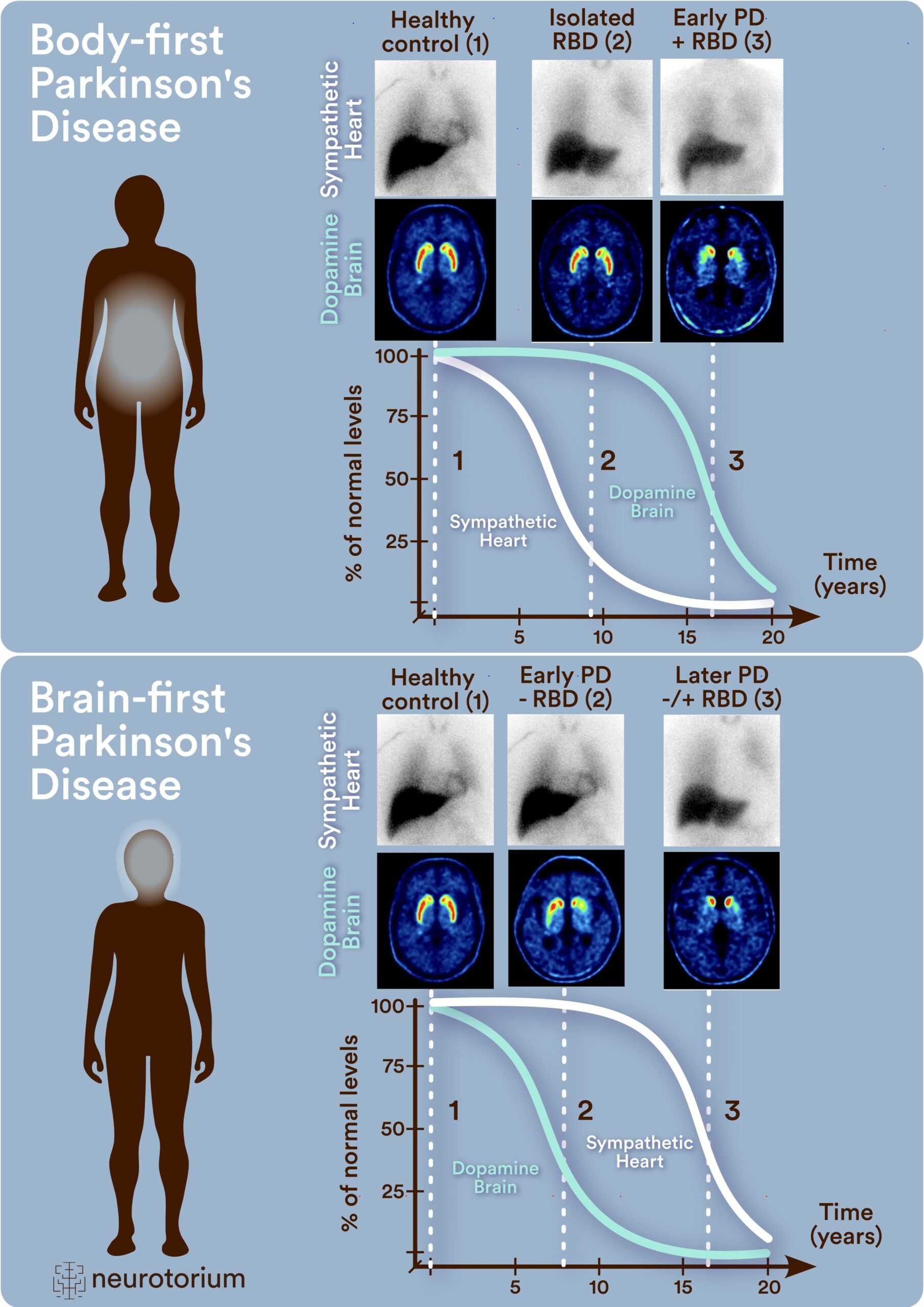
Figure 3: Trajectories of Neurodegeneration in Body- and Brain-First Subtypes of Lewy Body Disease
Trajectories of neurodegeneration in body- and brain-first subtypes of Lewy body disease. In body-first patients (top panel) the sympathetic innervation of the heart starts to degenerate 15-20 years before diagnosis. Prodromal patients with isolated RBD (iRBD) nearly all have severe cardiac denervation (invisble heart), but a normal or near-normal dopamine scan of the brain. When diagnosed with PD, these patients typically have a dopamine scan with rather symmetric loss in the putamen and an invisible heart. In brain-first patients (bottom panel), the dopamine system starts to degenerate early. At the time of PD diagnosis, these patients often shown quite asymmetric dopamine loss in the putamen, but most patients still have a normal or near-normal heart scan. A few years later, brain-first patients will start to show loss of the cardiac sympathetic innervation.
It can be estimated that it takes approximately 8-10 years for the heart to become invisible on MIBG scans (based on data from Tsujikawa et al.33). It is also known that it takes on average 8 years for a prodromal iRBD patient to convert to clinical PD or DLB34. This means that in most body-first cases, the heart starts to degenerate 8-10 years or more before the dopamine system starts to decline, and 16-20 years before the patient is diagnosed.
Newly diagnosed PD patients without RBD and minimal autonomic problems (brain-first) have clearly pathological dopamine brain scans, but they typically show normal or near-normal MIBG heart scans (Figure 3, bottom panel). They also show normal colon transit time and volumes, near-normal cholinergic signal in the colon evidencing limited parasympathetic denervation, and normal integrity of the locus coeruleus on MRI scans.13,35-37 Collectively, this pattern shows that brain-first LBD at the time of diagnosis exhibits clear, measurable pathology in the top of the brainstem, where the dopamine neurons are located, but limited or no measurable neurodegeneration or dysfunction below this level. This aligns with the brain-first subtype of LBD, where pathology begins above the brainstem.
Of note, MIBG studies consistently demonstrate that all later stage PD patients display severely pathological scans, i.e. an invisible heart.38,39 Thus, severe degeneration of the cardiac sympathetic nerves seems to be inevitable and occurs in all LBD patients. In most body-first patients, this degeneration starts more than 16 years before diagnosis, whereas in most brain-first patients, the cardiac degeneration develops after diagnosis.
In most body-first cases, the heart starts to degenerate 8-10 years or more before the dopamine system starts to decline, and 16-20 years before the patient is diagnosed.
Professor Dr. Per Borghammer explains the brain-first vs body-first model of Parkinson’s disease, which consists of two distinct pathways of disease progression starting from the gut, or nose. Learn how these findings could potentially pave the way for personalized medicine and new treatments to stop Parkinson’s disease in its tracks.
Learn how these findings could potentially pave the way for personalized medicine and new treatments to stop Parkinson’s disease in its tracks.
Postmortem Brain- and Body-First
In 2003, a landmark hypothesis was proposed by the German neuropathologist Heiko Braak.40-42 In short, this model suggested that Lewy pathology in all cases of PD initially appears in the gut and in the olfactory bulb. However, it was proposed that the olfactory pathology was not significant, since it did not spread very far. The Braak model therefore postulated that the earliest defining pathology is that in the parasympathetic nucleus at the bottom of the brainstem, from where it climbs sequentially upwards, reaching the dopamine cells, and eventually the cortex.
Following the Braak model’s publication, studies revealed that many early-stage postmortem cases lacked pathology in the parasympathetic nucleus but exhibited it in the limbic system, olfactory bulb, and upper brainstem.43,44 This was taken as evidence that not all cases followed the spreading pattern predicted by the Braak model.
A competing model was developed, which described brainstem-predominant and limbic-predominant neuropathological subtypes.45 However, this model suggested that Lewy pathology in all cases of LBD originates in the olfactory system and never in the gut.46-48 This alternative interpretation is also very difficult to reconcile with clinical and imaging evidence reviewed above. For this hypothesis to be true, Lewy pathology originating in the olfactory system would have to spread to the sympathetic postganglionic neurons, which is almost at the other end of the nervous system, leading to complete degeneration of this system over a 10-year period, while leaving the next-door neighbour, the highly vulnerable dopamine system, unharmed for a decade or more. The BvB model can be seen as a fusion of these two previous models. In body-first LBD, the first pathology is triggered in the gut, and spreads via the vagus nerve to the parasympathetic nucleus in the brainstem as proposed by Braak, but also via the sympathetic nerve fibres to the paravertebral ganglia, which is how the pathology reaches the heart so early.4 Animal studies have demonstrated that upon injection of Lewy pathology-like material in the gut of rodents, the pathology spreads equally well via the vagus and the sympathetic system, and that the pathology in the ganglia and heart most likely comes via the sympathetic route.49,50 In brain-first LBD, the pathology is triggered in the olfactory system or sometimes originates in the amygdala or other brain structures. The pathology then spreads via the connectome in the opposite direction of that seen in body-first cases.
Gradients in Postmortem Studies
An important yet often overlooked aspect of the BvB model is the concept of Lewy pathology gradients. This concept builds on the assumption that Lewy pathology displays certain characteristics. First, that the pathology starts very localized and spreads across synapses to connected neurons. Second, that the pathology builds up in each affected nucleus over time. If these assumptions are correct, gradients of pathology would be expected to emerge, and to be clearly discernible at the early stages of LBD before the brain is saturated with pathology and before significant neuron death has occurred.
Early body-first cases would be expected to show most pathology in peripheral sympathetic autonomic ganglia and at the bottom of the brainstem, and then progressively less pathology in the upper brainstem and limbic system. Early brain-first cases would show most pathology in the olfactory bulb and amygdala, less pathology in the lower brainstem, and little or no pathology in peripheral autonomic ganglia. These two overarching types of graded Lewy pathology have been clearly demonstrated in several, recent postmortem studies.11,12,51 Moreover, the proportion of cases with these two opposing gradients is approximately 50/50. It should be noted that less than 10% of postmortem cases show aberrant patterns, i.e. they represent “rare exceptions”, whereas the two opposing gradients represent “the rule” in postmortem studies.
The presence of these gradients in early incidental Lewy body disease is very compatible with the BvB model. It is also very compatible with the two opposing phenotypes seen in imaging studies and clinical symptoms. In contrast, these two gradients seem difficult to explain if Lewy pathology in all cases started in the gut40 and likewise, if it in all cases started in the olfactory bulb.45
Other authors have suggested alternative models, which is built on the idea that Lewy pathology does not spread from neuron to neuron, but rather arises in neurons due to cell-autonomous factors, induced by triggers coming via the blood stream, or arising in the dopamine-motor cortex circuitry.52-55 However, such models are also difficult to reconcile with the two opposing gradients seen at postmortem. Blood-borne factors could in principle trigger the first Lewy pathology anywhere in the brain, and “multi-focal” cases would also be expected to occur, i.e. cases with restricted pathology in far removed, non-connected brain regions.
This is not what the postmortem evidence shows. The two opposing gradients explained above seem to be much more stereotypical and non-random. They point to the olfactory bulb and peripheral autonomic neurons being the first affected structures in most cases of LBD. By extension, this suggests that the first Lewy pathology is not triggered by blood-borne factors, but by factors affecting the epithelium in the gut and nose, which could include toxins (e.g. pesticides), infections, and inflammation.7
The two opposing gradients explained above seem to be much more stereotypical and non-random. They point to the olfactory bulb and peripheral autonomic neurons being the first affected structures in most cases of LBD.
Dementia
As mentioned above, a large number of clinical studies show that body-first symptoms, including RBD, constipation, and orthostatic hypotension are much more common in prodromal DLB compared to prodromal PD. Also, in patients diagnosed with PD, the presence of these body-first symptoms at the time of diagnosis is a risk factor for faster progression towards dementia.56-58 This suggests, perhaps somewhat counterintuitively, that body-first LBD leads to more rapid dementia than brain-first disease. There may be several explanations for this.
The BvB model proposes that body-first LBD is inherently a more symmetric brain disease, since Lewy pathology arising in the gut may spread in a symmetric manner via the left and right vagus nerve and sympathetic connections.4 This is corroborated in animal models.59,60 Also, most imaging studies report that body-first PD and DLB patients show more symmetric dopamine loss on imaging compared to brain-first cases,61-68 although a single study did not corroborate these findings.69 Of note, no postmortem studies have systematically explored right-left asymmetries of Lewy pathology, since all modern brain banks conduct histology on single hemispheres, since the other hemisphere is fresh frozen for other types of analyses.
If correct, the more symmetric involvement of both hemispheres in body-first disease means that these patients have less reserve capacity compared to brain-first cases. Also, at the time of diagnosis body-first cases have profound (and possibly more symmetric) involvement of several key modulatory systems, including the raphe nuclei, locus coeruleus, pedunculopontine nucleus, and cholinergic basal forebrain. Dysfunction in these subcortical systems may contribute to slower cognition, impaired attention, fatigue, sleep and mood disorders. They may also serve as an efficient mechanism for spreading Lewy pathology across the central nervous system, since these systems collectively innervate the entire brain in a diffuse manner. Thus, severe involvement of these systems in body-first LBD may lead to faster limbic and neocortical Lewy body disease affecting both hemispheres. These arguments are all speculative, but can be tested in animal models, left-right hemisphere comparisons in postmortem studies, and especially, once an alpha-synuclein PET tracer becomes available.
Conclusion
Patients with LBD exhibit significant heterogeneity in symptom burden and disease progression. Accumulating evidence support that there is more than one subtype of LBD. These subtypes are probably caused by variable risk factors, triggers, and other pathogenic mechanisms. Improved understanding of LBD subtypes and the underlying causative mechanisms is necessary to pave the way for subtype-specific disease-modifying therapies in the future.
The body-first and brain-first hypothesis of LBD is a recently proposed theoretical disease model, which attempts to account for some of the variation seen among patients by focusing on the plausible origin sites and spreading patterns of aggregated alpha-synuclein. Although the model seems to have some explanatory power, it is likely an imperfect approximation at best and needs to be further validated and refined.
It is important to note that individual vulnerability factors including different genetic risks impact on the disease course among patients. Some patients may have neurons that are more vulnerable to intracellular Lewy pathology, and they would conceivably progress faster than patients with more resilient neurons, even in the presence of identical amounts of Lewy pathology. Improved understanding of such mechanisms will also identify novel treatment targets that can be explored in clinical trials.
Improved understanding of LBD subtypes and the underlying causative mechanisms is necessary to pave the way for subtype-specific disease-modifying therapies in the future.
Related content
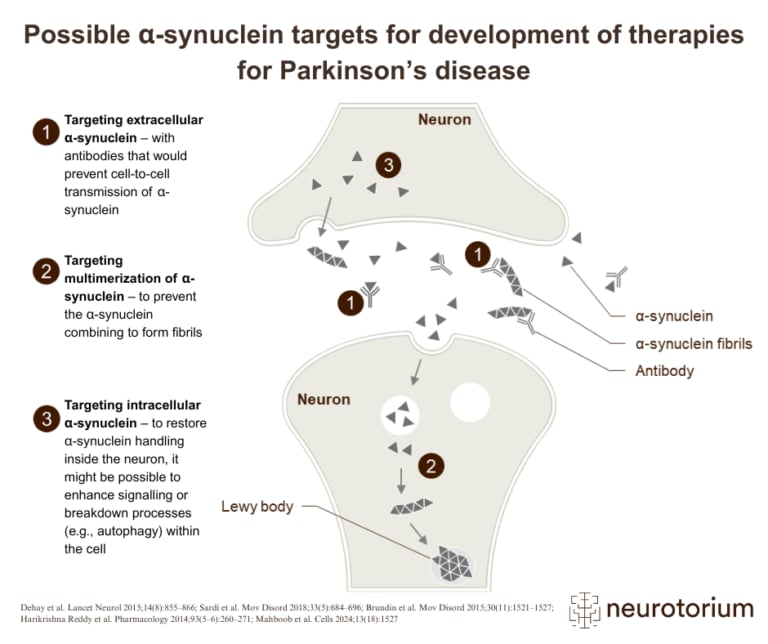
Overview of three therapeutic strategies targeting alpha-synuclein in the development of disease-modifying treatments for Parkinson’s disease
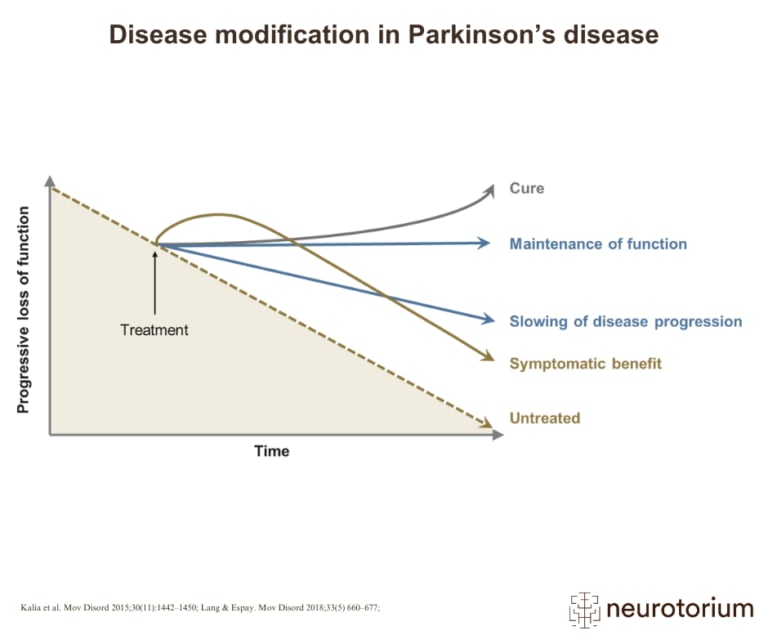
Graphical representation of how various treatment strategies can impact disease progression in Parkinson’s disease, from symptom relief to potential cure
{kind=link}
{kind=link}
{kind=link}
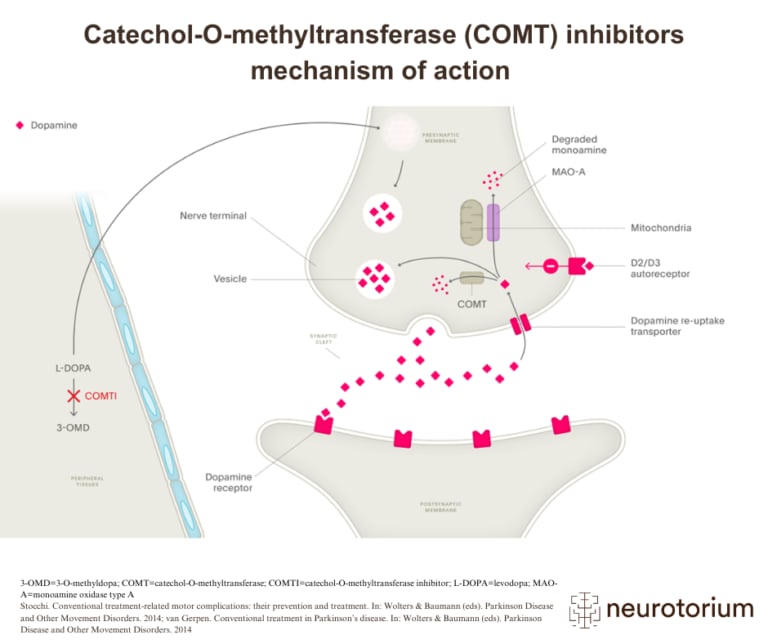
Illustration of how COMT inhibitors increase dopamine availability in Parkinson’s disease by preventing the breakdown of L-DOPA