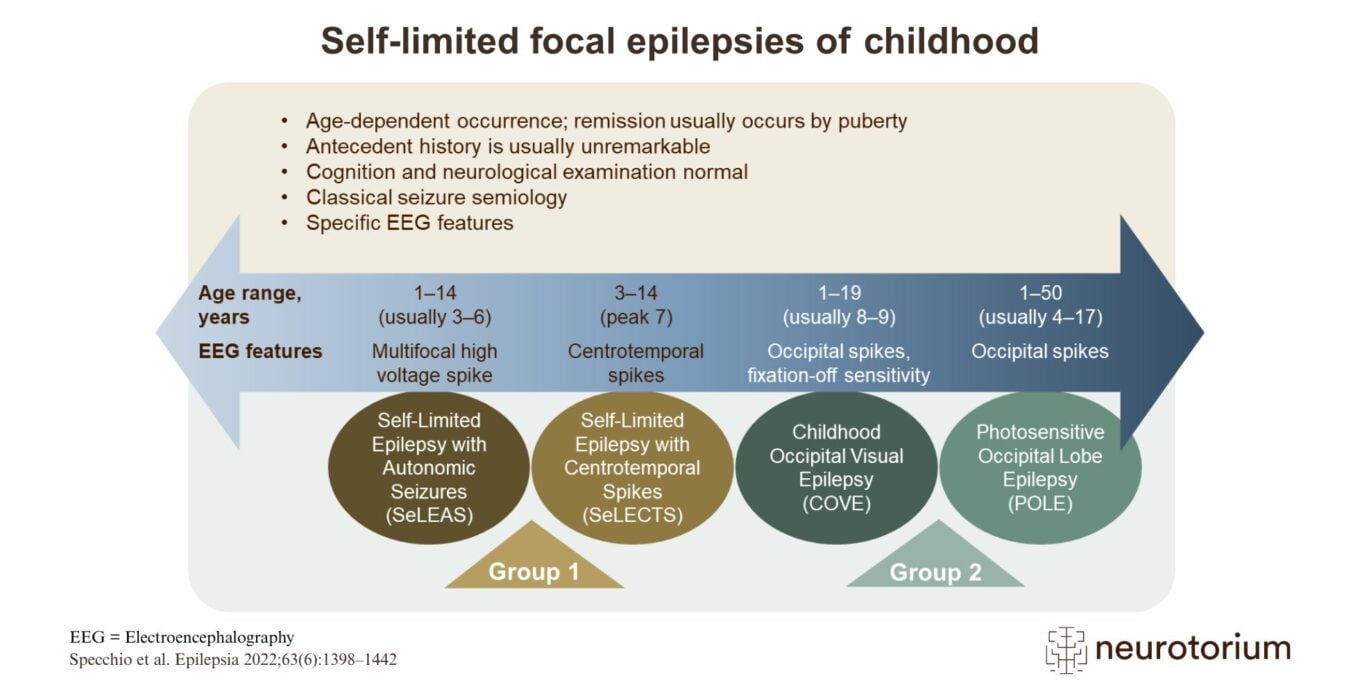
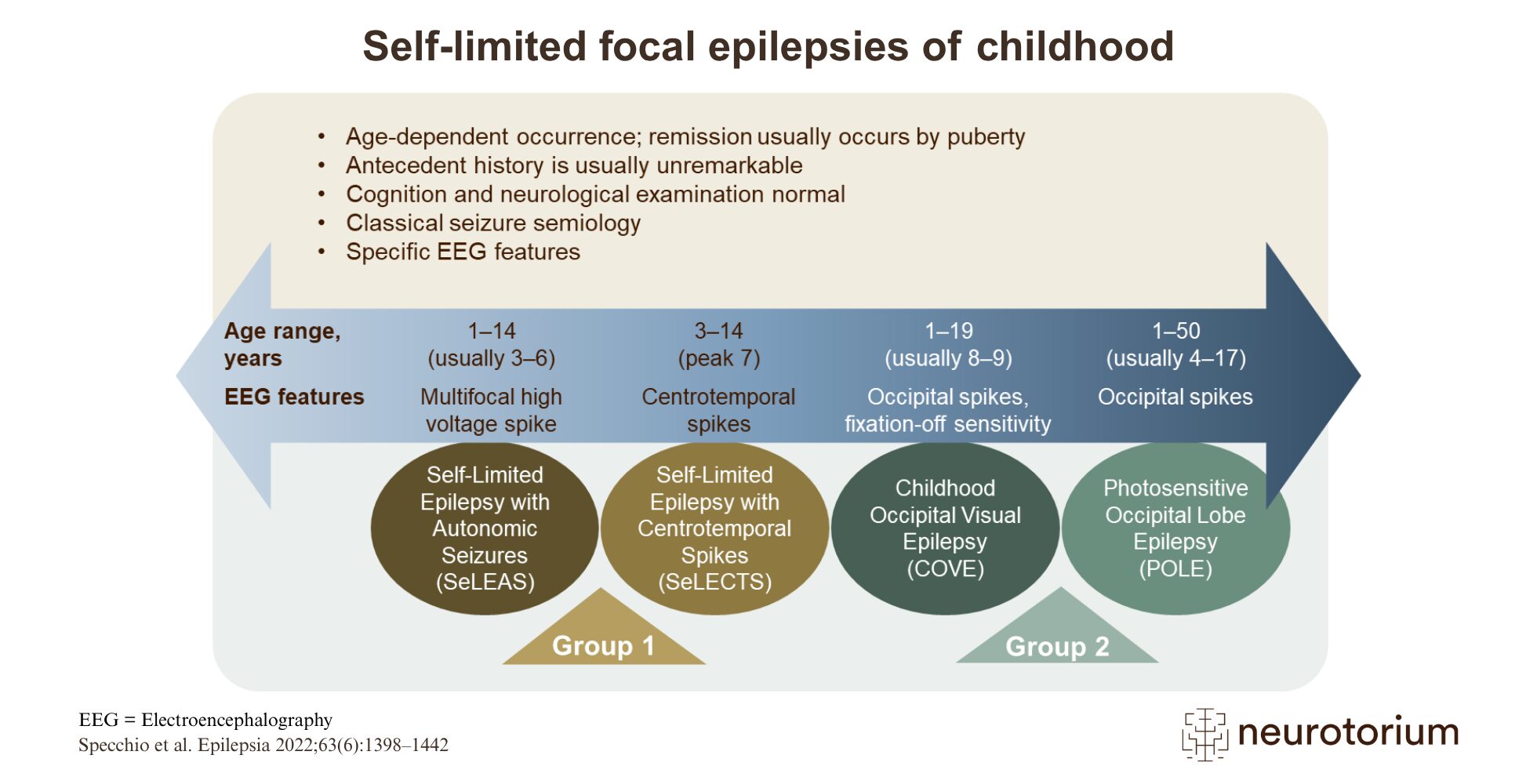
Self-limited focal epilepsies of childhood (SeLFEs) are a group of conditions occurring without a known cause in children who appear cognitively and neurologically normal and have no significant structural brain lesion.1 Genetic factors are presumed to play an important role in SeLFE development, but no specific genetic variants have been identified so far.1 The SeLFEs account for up to 25% of all paediatric epilepsies.1 Each syndrome has a specific age-dependent occurrence, with classic seizure semiology (focal motor or sensory seizures with or without impaired awareness which may evolve to bilateral tonic–clonic seizures) and specific electroencephalogram features, including epileptiform abnormalities with distinctive morphology and location, often activated by sleep.1 Most children with SeLFEs have features characteristic of one specific syndrome, but occasionally the features may be mixed, or one SeLFE type may develop into another.1 SeLFEs respond to pharmacological treatment.1
Two levels of syndromes are recognized, depending on the long-term prognosis.1 Remission is expected in all children with Group 1 epilepsy conditions.1 In Group 2 epilepsy conditions, remission is highly likely; however, in some patients, seizures may persist after adolescence.1
Related content
In this video, Professor Dr. Nathalie Jetté reviews depression as a common yet often under-recognized comorbidity in epilepsy.
In this video, Professor Dr. Gretchen Birbeck examines epilepsy-associated stigma as a global public-health challenge
{kind=link}
In this video, Professor Dr. Jacqueline French reviews practical, first-line decision-making for anti-seizure medication selection