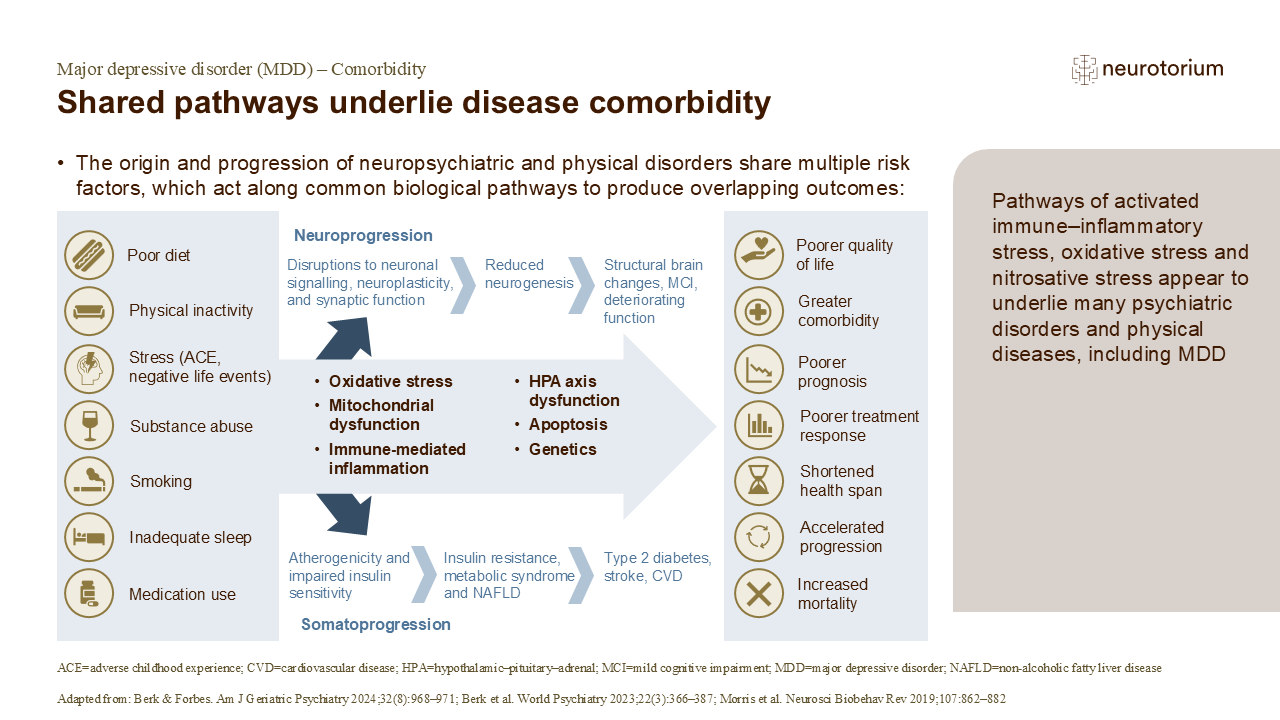
Mitochondrial function (i.e., ATP production) is impaired in people with MDD compared with controls, leading to inefficient respiration and the production of reactive oxygen species, resulting in oxidative stress.2 In addition, MDD has neuroendocrine effects, including sympathetic nervous system activation and HPA axis dysregulation, which can cause hypertension, hypercholesterolemia, hypertriglyceridemia, endothelial dysfunction and abdominal obesity, increasing the risk of diabetes and cardiovascular disease.4 MDD is also associated with chronic low-grade inflammation, with elevated levels of interleukin (IL)-1, IL-6, tumour-necrosis factor (TNF)-alpha, and C-reactive protein;3,4 this inflammation also underlies many different somatic diseases, such as diabetes, stroke, heart disease, cancer, and autoimmune disorders such as multiple sclerosis and rheumatoid arthritis.2,4 The inflammatory processes in MDD along with physical comorbidities, neuroendocrine effects of MDD and behavioural/lifestyle risk factors form a self-perpetuating loop, impacting the development, severity, prognosis and outcomes of MDD as well as its comorbid disorders.4
Focusing resources and interventions on those people most at risk of ill health (including people of low socio-economic status) to interrupt the cycles of neuroprogression and somatoprogression, e.g., through lifestyle interventions, may reduce the development of multiple comorbidities and enhance the quality of life and longevity for these patient populations.2