


Overview and Epidemiology
Chapter 6 in the International Classification of Diseases (11th edition; ICD-11)1 describes “Mental, behavioral and neurodevelopmental disorders” and thus, includes disorders due to substance use and addictive behaviors. According to the World Health Organization (WHO), these are “mental and behavioral disorders that develop as a result of the use of predominantly psychoactive substances, including medications, or specific repetitive rewarding and reinforcing behaviors”.1 The ICD-11’s category “Disorders due to addictive behaviors” includes “Gambling disorder” and the new diagnostic category “Gaming disorder”.2 Importantly, the ICD-11 is currently available in 7 languages (Arabic, Chinese, English, French, Portuguese, Russian, and Spanish), and thus, some countries may be slower to implement the new changes in diagnosing behavioral addiction.
A recent analysis of the global prevalence of mental health and substance use disorders (SUDs)3 yielded a worldwide prevalence of SUDs of 2.2%, with a higher prevalence of alcohol-use disorders (1.5%) compared to other drug-use disorders (0.8% total, including cannabis 0.32%; opioid 0.29%, amphetamine 0.10%; cocaine 0.06%), with higher levels of SUDs in high-income countries than in lower-income countries.
Another recent meta-analysis4 estimated prevalence rates of behavioral addictions around:
- 10.6% for internet addiction,
- 30.7% for smartphone addiction,
- 5.3% for gaming addiction,
- 15.1% for social media addiction,
- 21% for food addiction,
- 9.4% for sex addiction,
- 7% for exercise addiction,
- 7.2% for gambling addiction,
- 7.2% for shopping addiction.
A recent analysis of the global prevalence of mental health and substance use disorders (SUDs)3 yielded a worldwide prevalence of SUDs of 2.2%
Since the period covered fell into the COVID-19 pandemic, the authors stated that during the lockdown periods, the prevalence of food addiction, gaming addiction, and social media addiction was higher compared to non-lockdown periods. A recent study5 across 15 countries from Europe, America, and Asia showed that problematic internet usage was slightly lower in European countries compared to Asia (rates ranged from 1.1% in Finland to 10.1% in the UK, compared to 2.9% in Canada and 10.4% in the US). There were differences in specific problematic internet usage rates, e.g., problematic gaming ranged from 0.4% in Poland to 4.7% in Indonesia.
Another review6 on digital addiction estimated that up to ¼ of the population could be affected by at least one subtype of digital addiction; i.e., global pooled prevalence was 26.99% for smartphone addiction, 14.22% for Internet addiction, and 6.04% for game addiction. There was considerable geographical variation, with low/lower-middle income countries having a higher burden of digital addiction and higher prevalences among men than women regarding internet addiction and game addiction.

Psychiatric Comorbidities
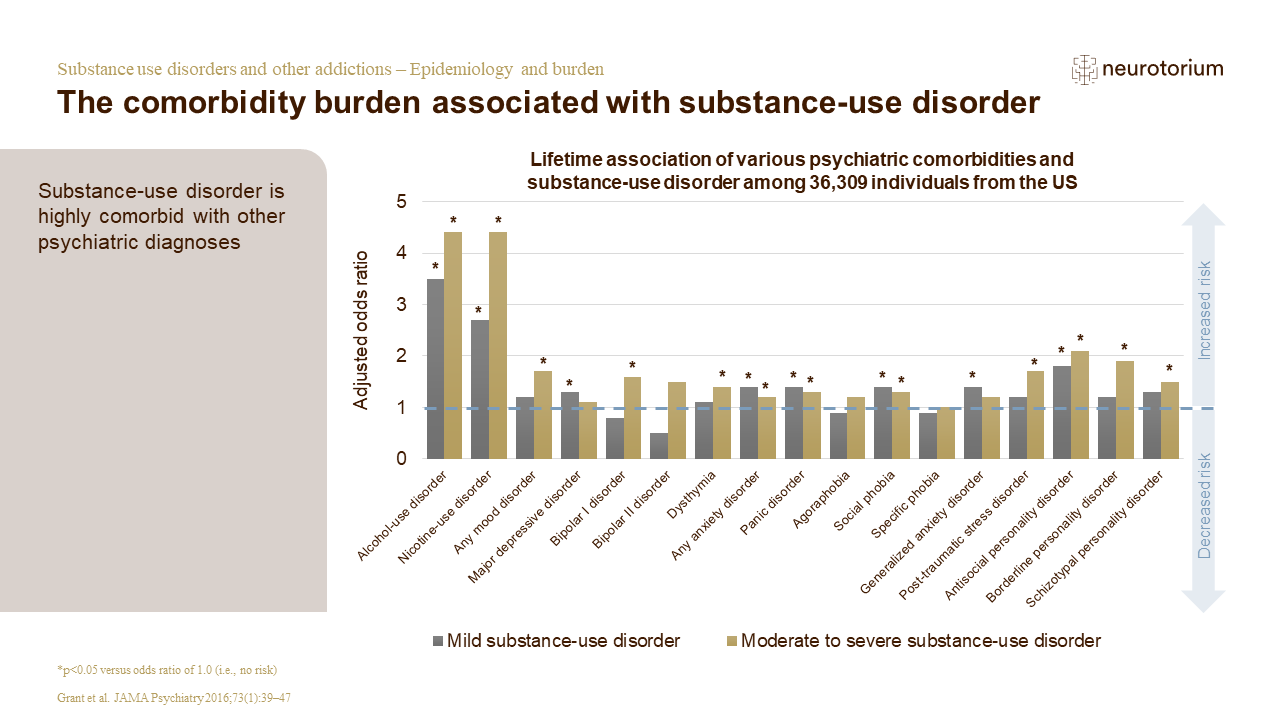
People with SUDs frequently suffer from multiple conditions at a time, i.e., they might have mental or physical health comorbidities or both in addition to their addictive disorder. Studies report a high prevalence (i.e., around at least 50%) of psychiatric comorbidity among people with SUDs.9-11 The high prevalence of dual disorders may be attributed to common risk factors that can contribute to both mental illness and substance use and addiction, such as genetic factors, epigenetic influences, environmental factors, stress, trauma, and adverse childhood experiences, as well as the involvement of the same brain regions.11
The high prevalence of dual disorders may be attributed to common risk factors that can contribute to both mental illness and substance use and addiction
Despite the fact that SUDs are mental health disorders (see ICD-11)1, some authors view and treat them as completely separate conditions: Mental disorders may contribute to SUDs, and substance use, and addiction can contribute to the development of a variety of other mental disorders.11 Very common are affective disorders (which include generalized anxiety disorder, panic disorder, and post-traumatic stress disorder, depression and bipolar disorder), attention-deficit hyperactivity disorder (ADHD), psychotic illness, borderline personality disorder, antisocial personality disorder and other substance use disorders.11 The overlap is especially pronounced with serious mental illness (SMI), i.e., a diagnosable mental, behavior, or emotional disorder that causes serious functional impairment that substantially interferes with or limits one or more major life activities (e.g., major depression, schizophrenia, or bipolar disorder); approximately 1 in 4 individuals with SMI also have an SUD.
Psychiatric comorbidity is frequent among patients with behavioral addictions as well. A meta-analysis13 found significant and positive associations between internet addiction and alcohol use disorder (AUD), ADHD, depression and anxiety. ADHD rates appear to be particularly high among people with behavioral addictions, with studies reporting rates up to over 88%.14
Burden of Disease
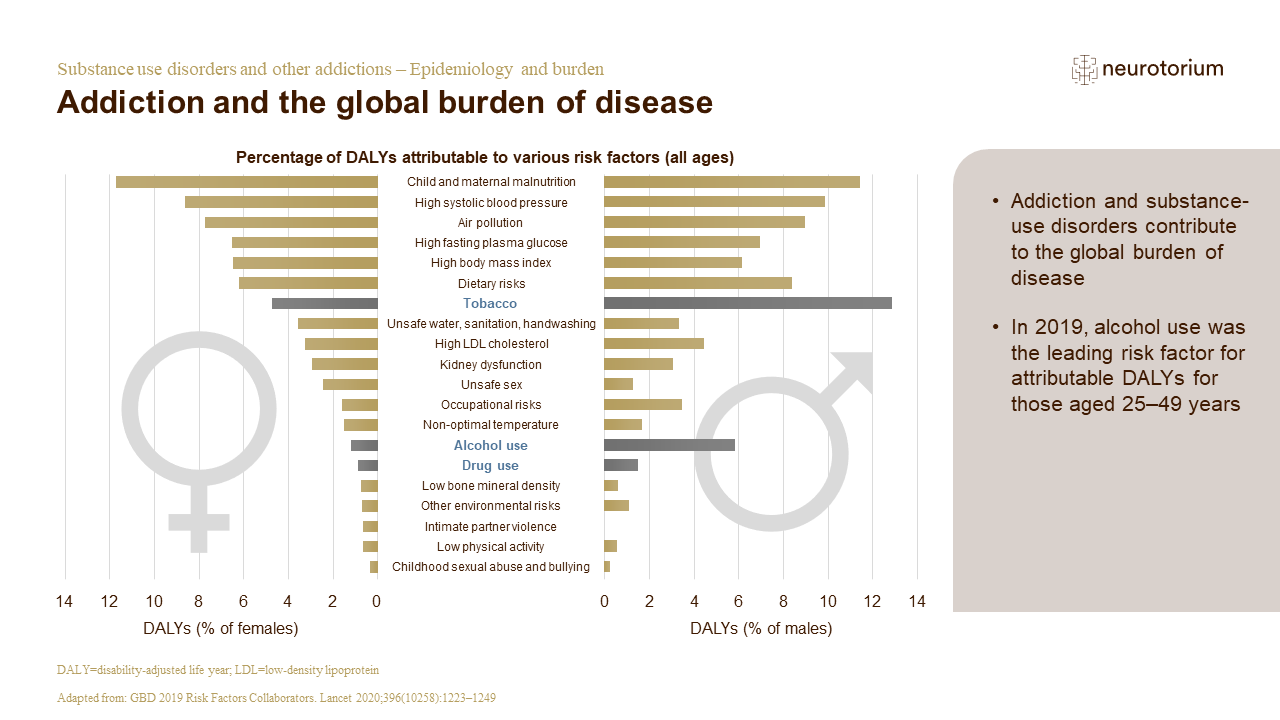
In a global burden of disease study from Australia that aimed at estimating global disease burden attributable to alcohol and drug use between 1990 and 2016 for 195 countries and territories, alcohol use disorders (AUDs) were the most prevalent of all SUDs, with over 100 million estimated cases, followed by cannabis dependence (22 million cases) and opioid dependence (27 million cases).15 In 2016, 99 million disability-adjusted life-years (DALYs) and 4.2% of all DALYs (3.7–4.6) were linked to alcohol use, and 32 million DALYs (27.4–36.6) and 1.3% of all DALYs (1.2–1.5) were to drug use as a risk factor.15
The burden of disease varied substantially across regions, whereas the impact of substance use on other health outcomes played a major role. Interestingly, the alcohol-attributable burden was highest in countries with a low and high-middle socio-demographic index (SDI), whereas the burden due to drugs increased with a higher SDI level. Notable were also the almost 21 million DALYs due to injuries attributable to alcohol use per year, with almost half of those related to self-harm and interpersonal violence, followed by transport injuries and unintentional injuries. Almost 2 million DALYs per year were attributable to drug use and self-harm.
Notable were also the almost 21 million DALYs due to injuries attributable to alcohol use per year, with almost half of those related to self-harm and interpersonal violence
There is also a noteworthy sex difference regarding disease burden for most substances, with a sex ratio of up to 4 to 1 (men to women). Most likely, this difference is linked to regional variation in social acceptability and cultural norms and regulations of drug and alcohol use and its impact on lifetime exposure.17
Behavioral addictions also entail considerable disease burden:19 For example, “problematic usage of the internet”, i.e. addictive, hazardous, harmful and unsafe use, includes internet addiction (covering Gaming Disorder, Social Network Use Disorder, Online Shopping Disorder or Online Pornography Viewing Disorder), has been associated with mental health disorders (such as ADHD, other SUDs, social anxiety disorder, obsessive-compulsive symptoms, hostility/aggression and personality disorders), physical health consequences (e.g. back pain, sleep problems, or migraines), as well as reduced cognitive control and social functioning poor school performance and lack of productivity.
Benefits of Preventing SUD
Prevention of SUDs is key to preventing considerable harm and the burden of disease to individuals, families, communities, and society. Prevention may be universal, i.e., offered to an entire population regardless of their level of risk; selective, i.e., targeting groups at risk; or indicated, i.e., offered to individuals already experiencing symptoms.20
The 3 types of prevention thus can take place prior to substance use issues (primary prevention), when problems arise (secondary prevention/early intervention and treatment), or to mitigate harmful effects of substance use (tertiary prevention/harm reduction).21 Prevention may facilitate early diagnosis and treatment of underlying (co-)morbidities and subsequently help prevent development of a SUD, or yield initiation of evidence-based treatment of the disorders.
Prevention may be universal, i.e., offered to an entire population regardless of their level of risk; selective, i.e., targeting groups at risk; or indicated, i.e., offered to individuals already experiencing symptoms.20
Conclusions
Given the current scope of SUDs, including behavioral addictions, which are of particular concern among young people,22 research and funding of preventive and early intervention measures are essential. With new possibilities, new risks arise, and new skills need to be learnt. In this case, the reasonable and targeted use or self-management skills regarding internet usage for professional and private purposes need to be learnt and practiced.
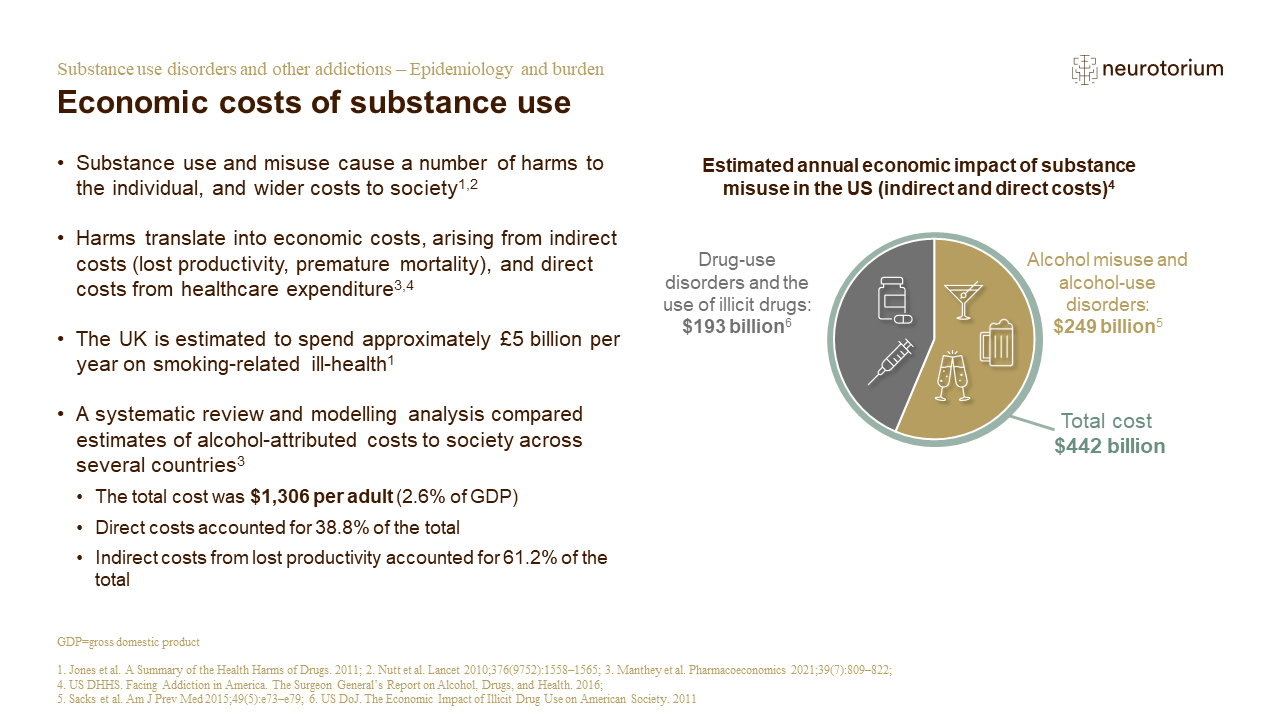
Only 1 in 10 individuals with SUDs receive specialized treatment despite the known huge cost savings of treatment and prevention measures.23 We know from the literature that early intervention pays off not only economically, but also regarding clinical outcomes as the progression of disease might be altered. For example, especially for ADHD, studies show that earlier intervention/treatment with stimulants in children might prevent future substance use problems.24,25
Finally, addressing addiction falls into the realm of providing mental healthcare and promoting mental and overall health. Global mental health movements have been emphasizing the promotion of human rights in mental health care in accordance with the UN Convention on the Rights of Persons with Disabilities (CRPD) and the WHO Quality Rights Initiative.26 Despite significant recent improvements in mental health service delivery, there is still -besides a general lack of treatment providers in some regions – substantial reporting of stigmatizing attitudes and human rights violations and abuse in mental health settings. Thus, developing new and better prevention, diagnosis, and early intervention measures also encompasses the promotion of a different narrative around and de-stigmatization of mental health and addictive disorders.
Only 1 in 10 individuals with SUDs receive specialized treatment despite the known huge cost savings of treatment and prevention measures23
Related content

Professors Christoph Correll and Gabriele Fischer discuss the challenges of managing co-occurring schizophrenia and substance use disorders, offering insights into this complex comorbidity.

Discover insights from Professor Gabriele Fischer on understanding relapses as part of substance use disorders, the importance of patient and family education, and the need to address comorbidities like depression, anxiety, and ADHD. Explore more about addictions at Neurotorium.org.

Substance-use disorders are common among people with bipolar disorder