

The technology of virtual reality
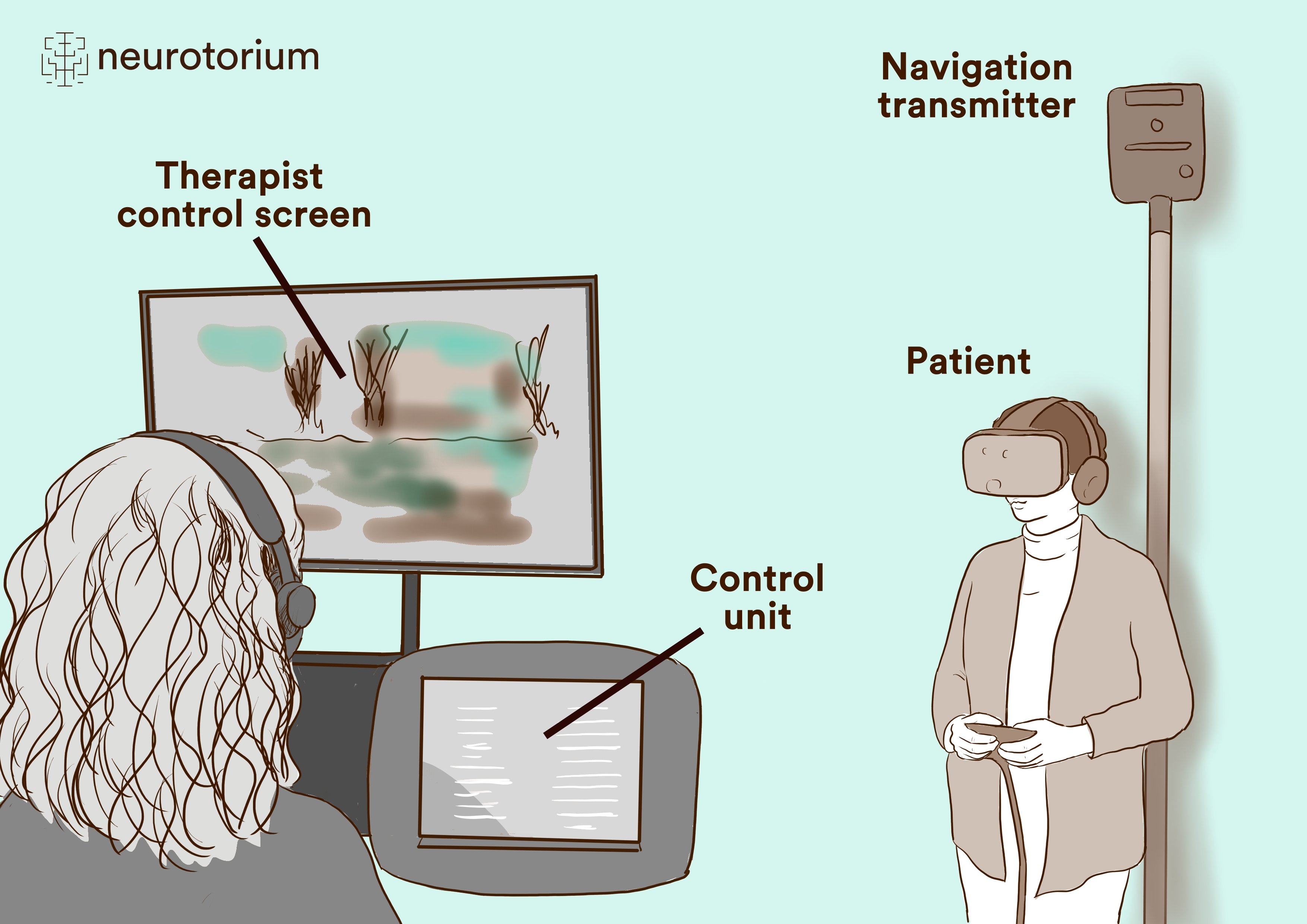
There are several technical ways to provide patients with this new therapeutic approach. VR can be created either through projection via a so-called head-mounted display or via large-scale screen projection.1 It is of central importance, that VR differs from other media in that this technology largely shields the user from external stimuli and offers a time-accurate simultaneous interaction with the virtual environment: Common VR systems detect user movements via sensors and adjust the field of view in real-time. A typical setup for exposure treatments using virtual reality is shown in Figure 1. It depicts the participant wearing a head-mounted display. Movement within the room is tracked by navigation transmitters. The therapist can view the patient’s perspective via the control screen. The joystick is used for additional actions, such as pushing buttons, opening doors, etc. (Fig.1).
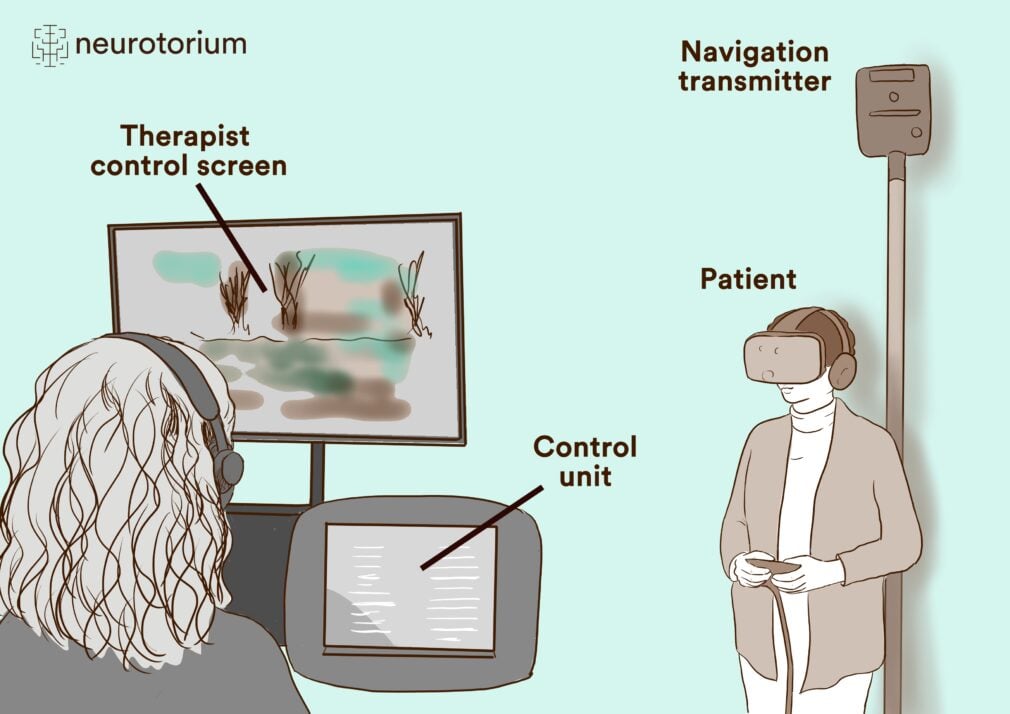
Figure 1: Virtual-Reality Setup
VR-Lab kbo-Inn-Salzach-Hospital, Wasserburg/Inn, Germany.
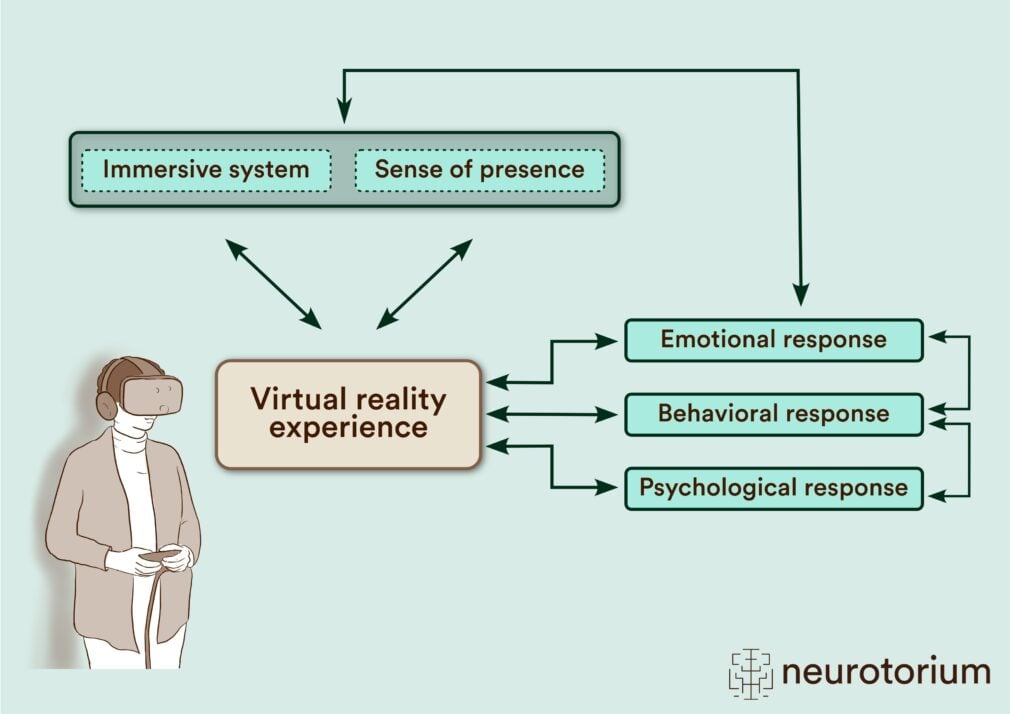
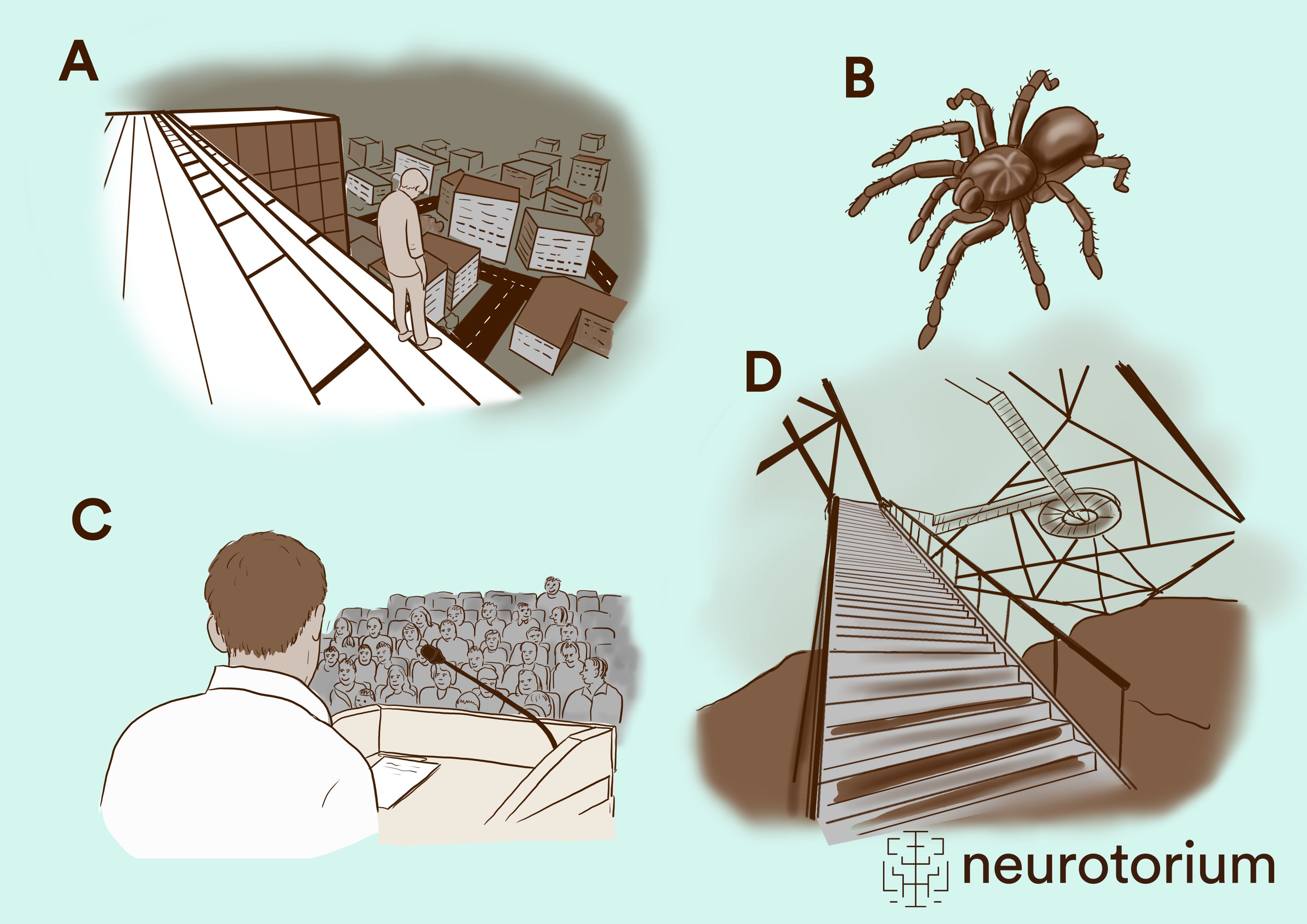
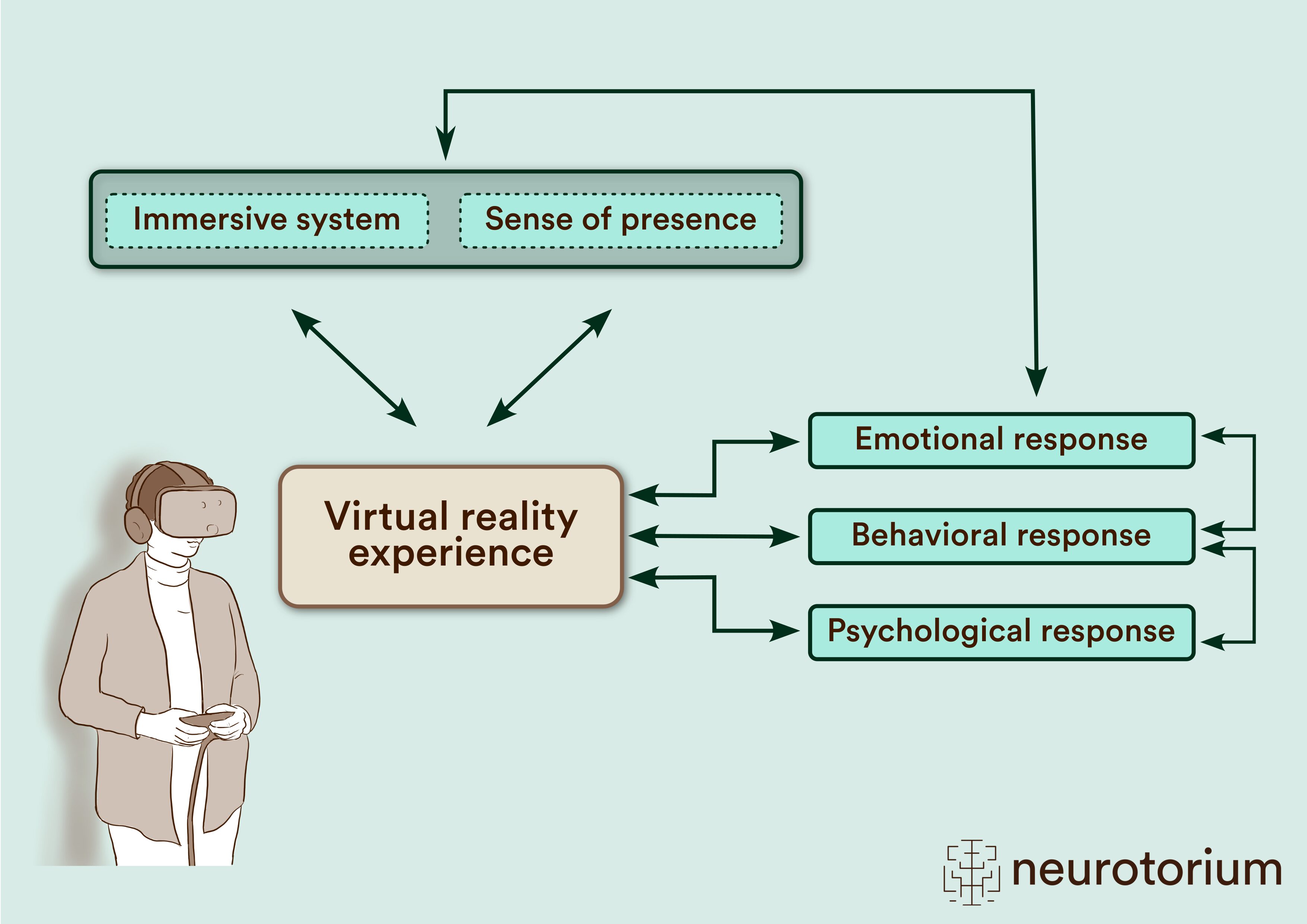
With regard to possible exposure scenarios, innovative software enables the generation of almost any environment (Fig. 2). The feeling of being in the virtual space is called presence. The technical features of the system that enable the virtual experience are referred to as immersion. While higher immersion generally leads to a more intense experience of presence, VR research shows also that presence and emotional experience are likely to influence each other. In particular, activating emotions such as fear are associated with a higher sense of presence. Also, the emotional response is interconnected both with the behavioral and the physiological response. In turn, all types of response are influenced by the virtual experience but also influence the virtual experience at the same time (Fig. 3).8
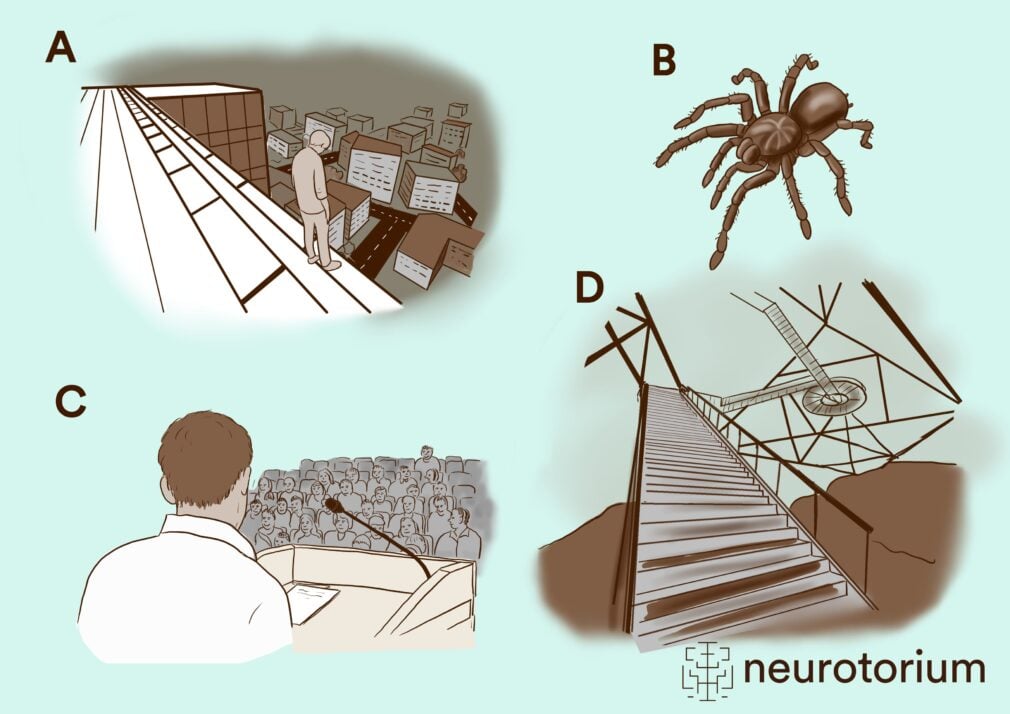
Figure 2: Various scenarios for exposure therapy in virtual reality for acrophobia (height fear)
(a, d), spider phobia (b), and social phobia (c)25.
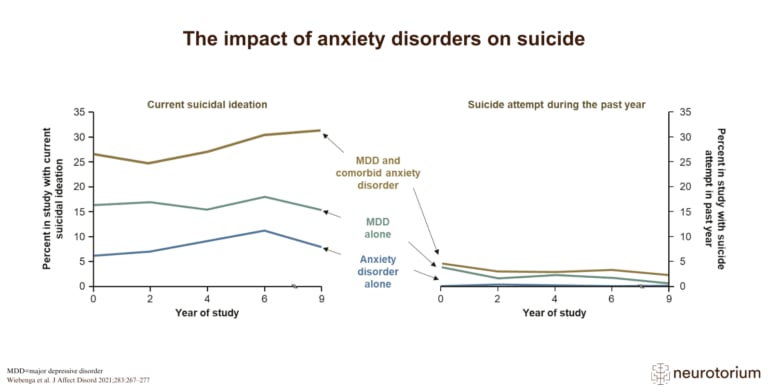
Interestingly, in the early stages of VR research there were concerns about VR’s ability to accurately simulate threatening stimuli to induce the necessary physiological responses along with the emotional component of anxiety. However, as revealed by an analysis of 39 studies investigating psychophysiological VR-associated fear responses in both patients with anxiety disorders and healthy individuals, VR exposure is indeed capable to provoke strong and sufficient psychophysiological arousal, especially with regard to electrodermal activity.9 In a study on acrophobia, during exposure heart rate increased in accordance with the emotional fear response in patients while in healthy subjects no change was observed.10
Effectiveness of VR in anxiety and comparison with in-vivo exposure
Numerous studies have examined the effectiveness of VRET (virtual reality exposure therapy) in anxiety disorders. Randomized controlled trials have primarily been conducted in phobic disorders, especially flight-, spider-, and acrophobia, as well as in panic disorder, agoraphobia, and social anxiety disorder. Meanwhile, several meta-analyses also suggest high effect sizes compared to waitlist control and indicate equivalent efficacy when compared to in-vivo treatment.11
As reported by van Loenen and colleagues, a meta-analysis of 16 trials including 817 participants and comparing VR-CBT vs. waitlist revealed a medium effect size (n=10; Hedges g=−0.490; 95% CI −0.82 to −0.16; p=.003) favoring the VR condition. Most importantly, the mean effect size of VR-CBT compared with in-vivo CBT exposure (n=13) was small and non-significant, suggesting equivalent effectiveness when in-vivo and in-virtuo exposure is compared.11 Similar results have been shown by Wechsler and colleagues (2019), who analyzed data from nine studies including specific phobia, social phobia and agoraphobia. In a comparison of VRET and in-vivo exposure, no significant differences emerged for specific phobia.12 Moreover, there is evidence for significant effects in social anxiety: In a narrative review, Seuling and colleagues (2024) shed light both on social anxiety disorder as well as public speaking anxiety. In an analysis of 20 studies, VRET proved to be a promising tool for the treatment of both social and public speaking anxiety offering an alternative and comparably effective approach to conventional exposure therapy.13 With a particular focus on public speaking anxiety, the implementation of VR in a conventional speakers’ training might thus be an interesting area of application apart from therapeutic use. Analyzing a total of 22 trials, Morina et al. (2023) discerned significant pre-post Hedges´ g effect sizes ranging between 1.20 (post treatment) and 1.06 at 12 months follow-up. When comparing VR and waitlist control, a significant effect size of 0.88 was reported. No significant differences were detected when VR exposure was compared with in-vivo treatment.14
Although further research is needed, the currently available studies overall suggest considerable clinical effectiveness of VRET. Given the recurring concerns about the limitations of the technology and the fact that every available VR scenario initially appears as a simulation, this is a remarkable finding. It once again suggests that ultra-highly realistic, expensive VR scenarios may not be strictly necessary for successful therapy. A study in acrophobia showed that even simple scenarios can induce a clinically relevant and statistically highly significant increase in subjective anxiety in patients with acrophobia compared to healthy controls. This increase was accompanied by statistically significant, though less pronounced, psychophysiological activation.10
Augmented reality (AR)
A promising method to further develop exposure-based therapies is the combination of VR with augmented reality (AR), referred to as mixed reality. Although VR and AR share many similarities, there are relevant differences: In VR, the user is completely immersed in a virtual world, while in AR the virtual stimulus is introduced into the real world. This strategy presumably increases the sense of presence and the realism assessment, which, as described above, is a key factor in inducing fear in exposure-based therapies. This difference between the two technologies enables AR to provide a markedly more realistic exposure-based therapy. On a technical level, AR is easier to implement, as only the relevant stimulus needs to be simulated, not the entire environment.15
The evidence base for AR is, however, considerably less extensive than that for VR (for review see Grimaldos et al., 2025).15 Nevertheless, some studies show that AR, like VR, produces noticeable anxiolytic effects that remain stable at follow-up. Botella and colleagues (2016) studied 63 patients with simple phobia and compared in-vivo exposure sessions with AR treatment. They reported that significant effects were obtained under both conditions. However, although initially patients benefited more from in-vivo exposure, the difference disappeared at follow-up assessments, and AR was comparable to conventional therapy.16 The use of AR in a smartphone app also appears to be effective: In a controlled study with patients with arachnophobia, the effects of AR were compared to a non-intervention group. A regular two-week self-administered treatment consisting of six sessions of 30 minutes each resulted in a significant superiority compared to the control group.17
New potential areas of application
One of the much-discussed advantages of VR is the ability to simulate situations, that might in fact be dangerous in reality, without risk. Apart from acrophobia, this might be especially helpful for patients with fear of driving a car, as exposure therapy can be limited or unfeasible at the beginning of treatment due to the high symptom load, for safety reasons. Case observations also suggest that patients can sometimes benefit within just a few sessions.18 In a controlled study, Kaussner and colleagues demonstrated that VR treatment administered in only five sessions could significantly improve the symptoms of patients with driving phobia.19
Innovative studies address the management of anxiety symptoms in certain life situations such as anxiety and avoidance behavior in medical care. According to a meta-analysis by Zeng et al. (2025),20 patients with perioperative anxiety, perinatal anxiety, fear of medical examination, and anxiety related to illness can benefit from VRET as well. This could be particularly relevant for the treatment of children. In a study involving 99 children, the authors investigated how VR coaching could reduce anxiety and stress before a hospital examination. It was shown that children who received specific VR coaching experienced up to 60% less anxiety than those in the control group. Remarkably, even parental presence was much less needed in the intervention group.21
Limitations and side effects of VR
It should be noted that VR simulation per se is not psychotherapy but rather a tool for clinicians. VR represents a new medium for conveying therapeutically useful information and stimuli, whose added value depends critically on its integration into a meaningful therapeutic context. For this reason, VR cannot replace a psychotherapist. Likewise, the use of VR in exposure therapy should not lead to the neglect of the usual adjunctive cognitive-behavioral therapy measures. This means that VRET has to be integrated into a comprehensive treatment plan from the outset, which, in addition to thorough cognitive preparation according to best practices, should also ensure that the effects achieved generalize to real-life feared situations.
VR can also cause unwanted side effects. The most well-known and significant side effect is “cybersickness” or “simulator sickness.” This includes symptoms such as nausea, dizziness, disorientation, which are most likely caused by irritation of the vestibular system and probably share a similar etiology with motion sickness. Mild forms of cybersickness may diminish over time with longer habituation and/or repeated practice, while more severe forms may require discontinuation of VR exposure. Symptoms of cybersickness usually subside quickly after the simulation ends; long-term effects are not known. The likelihood of cybersickness varies greatly depending on the patient population and the technology used, and a comprehensive assessment of influencing factors and corresponding recommendations has not yet been established.22
Future perspectives
Interesting perspectives arise from considerations regarding the combination of artificial intelligence (AI) and VR.23 In particular, treatment personalization and adaptation through data collection are seen as relevant factors. For example, new possibilities emerge through the integration of facial recognition software and systems that can quickly and in real-time detect stress, anxiety, or discomfort and trigger appropriate system responses. An important aspect of using AI in VR is automation, which can potentially save personnel resources by eliminating the need for instructions. In automated VR treatments, patients are typically guided by an avatar, and scenarios can be customized individually. There are already studies on the automation of VR for conditions such as acrophobia, fear of public speaking, spider phobia, and schizophrenia. However, there is also evidence that automation in VR might lead to a reduced emotional reactivity potentially associated with a reduced therapeutic effect.24
Further perspectives include the implementation of biofeedback systems that measure physiological signals like heart rate, muscle tension, skin conductance, and other parameters. Additionally, the integration of gamification elements into the VR environment is of interest, as it can increase engagement and willingness to participate in therapy. Feedback on specific challenges or rewards has already been incorporated into therapy programs (for review see Bell et al., 2024).1
Summary
VRET represents an effective and cost-efficient alternative to in-vivo exposure therapy. Given the limited personnel resources in psychotherapy and the high acceptance rates among patients, VR therefore might represent a potential standard module for integration into a comprehensive CBT-based treatment concept for anxiety disorders. Although studies and meta-analyses are available for a range of mental disorders, it should be noted that the data in anxiety disorders is currently by far the most extensive. The strongest evidence currently exists for specific phobias and social anxiety disorder. In combination with the integration of psychophysiological measurements, eye tracking, facial recognition, and the inclusion of AI, there are further prospects for optimizing this innovative form of therapy.
Declaration of interest:
P. Zwanzger has received speaker fees or honoraria for advisory board participation from Janssen Cilag/Johnson & Johnson, Schwabe, Sympatient, GAIA, MagVenture, Boehringer, Idorsia, Hennig, Lundbeck, Astrazeneca, Pfizer, BMS, Servier, and Neuraxpharm. He is a board member of the German Society of Psychiatry (DGPPN), Speaker of the DGPPN-Committee Digital Psychiatry and President of the German Society of Anxiety Research (GAF).
Related content
{kind=link}
{kind=link}
{kind=link}
Suicidal ideation is far more common than attempts in people with anxiety or depression, especially with comorbid disorders and severe depression.