
The hypothalamus–pituitary–adrenal (HPA) axis appears to be crucial in the development of the symptoms of depression.1 Patients with depression frequently have high circulating levels of cortisol,5 the hormone released from the adrenal cortex.4 Providing evidence for the connection from the other direction, patients with Cushing’s syndrome (characterised by a long-term increase in the levels of glucocorticoids, including cortisol)6 often show symptoms of depression, symptoms which are relieved when the cortisol overactivity is treated.5
Long term HPA overactivity has neurotoxic effects, particularly on the hippocampus.2 One proposed mechanism for the neurotoxic effects of cortisol is via the molecule BDNF (brain-derived neurotrophic factor), which normally sustains the viability of neurones.2,4 Chronic elevated cortisol reduces BDNF levels, which can lead to loss of neurones in the brain, particularly the hippocampus.2,3,4 Interestingly, treatment with antidepressants appears to restore the monoamine depletion seen as a result of chronic stress; this restoration can increase BDNF levels (and other trophic factors) and, potentially, restore some of the changes to the brain seen in depression.3,4
Related content
Treatment-resistant depression (TRD) represents a significant clinical challenge, affecting approximately 30% of individuals with major depressive disorder (MDD) who fail to respond to at least two adequate antidepressant trials.
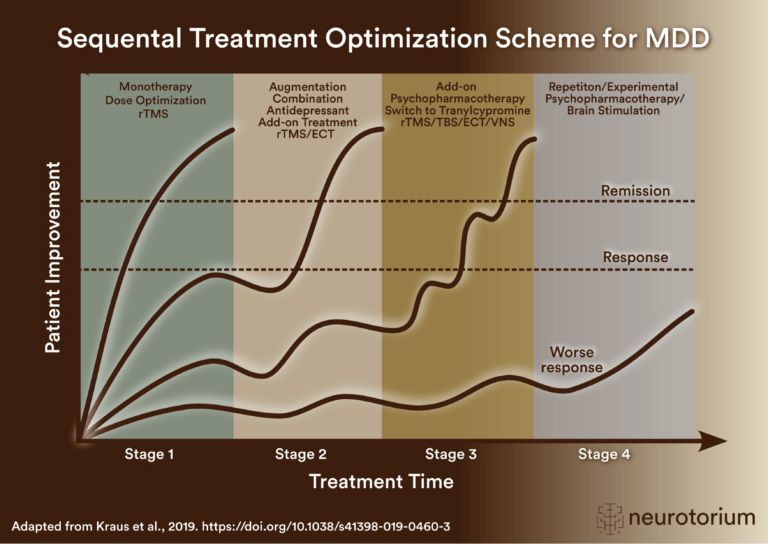
Sequential treatment optimization scheme for major depressive disorder generated according to international evidence.

Key steps for managing factors that may confound antidepressant treatment response, including dose, side effects, comorbidities, stressors, adherence, pharmacogenomics, interactions, and treatment algorithms.