
Introduction
Major Depressive Disorder (MDD) is a highly prevalent psychiatric condition with significant individual and socio-economic burden.1-3 Despite the broad availability of numerous effective therapeutic interventions, up to 30% of patients fail to achieve adequate symptom relief and are classified as having treatment-resistant depression (TRD).1-3
TRD is associated with higher rates of suicidality, chronicity, psychiatric and somatic comorbidities, and frequent hospitalizations.1,2,4 The heterogeneity in its definition, etiology, and treatment response makes TRD a complex challenge not only for affected individuals and their significant ones but also for clinicians and all experts involved in their treatment and care.1,2,5
Definition and Prevalence of TRD
A consensus definition of TRD has yet to be universally established, with different conceptual frameworks influencing epidemiological estimates.3,5,6 The most widely accepted definition, used in the majority of international studies and adopted by the FDA and EMA, characterizes TRD as the failure to respond to at least two adequate antidepressant trials despite optimal dosing and adherence.1,2
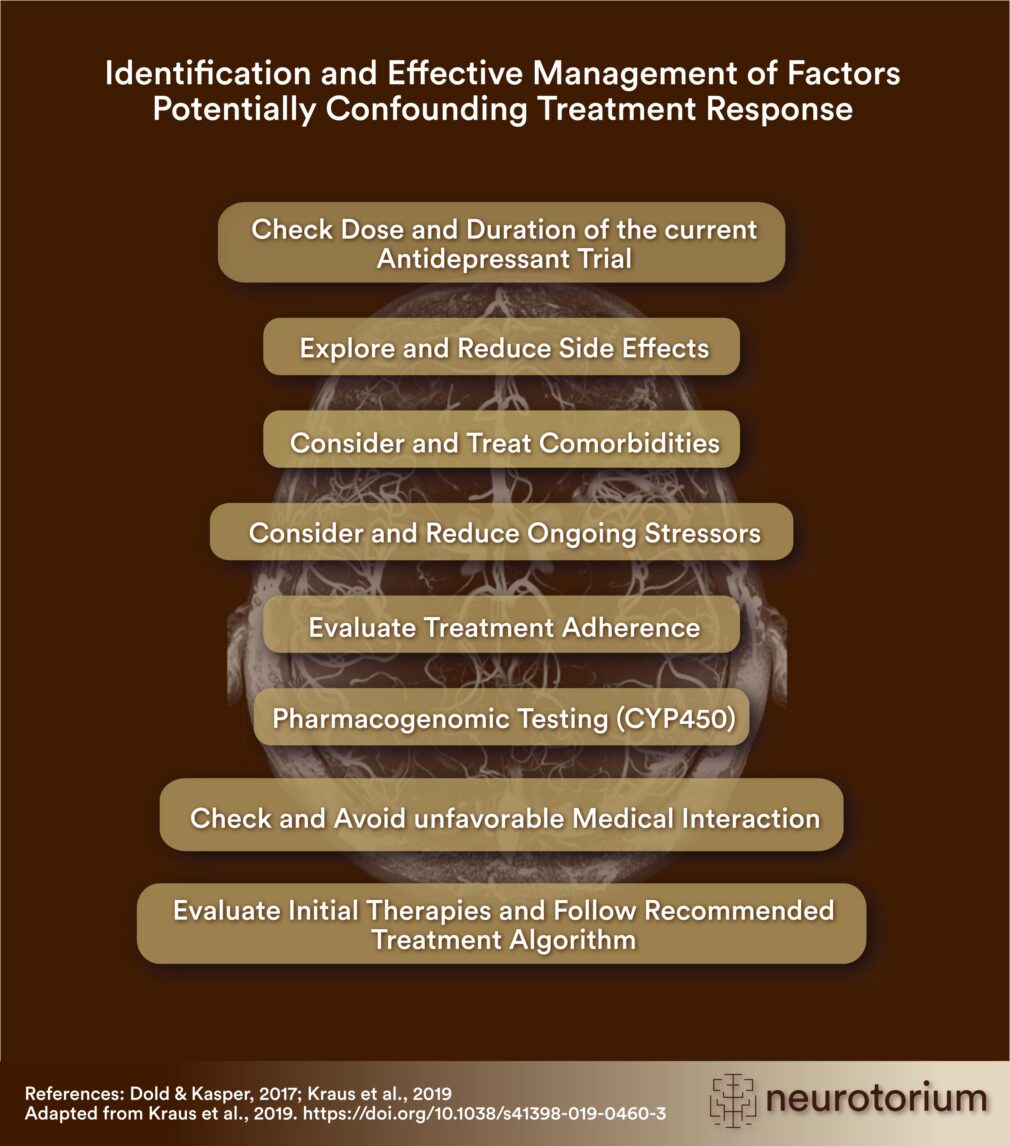
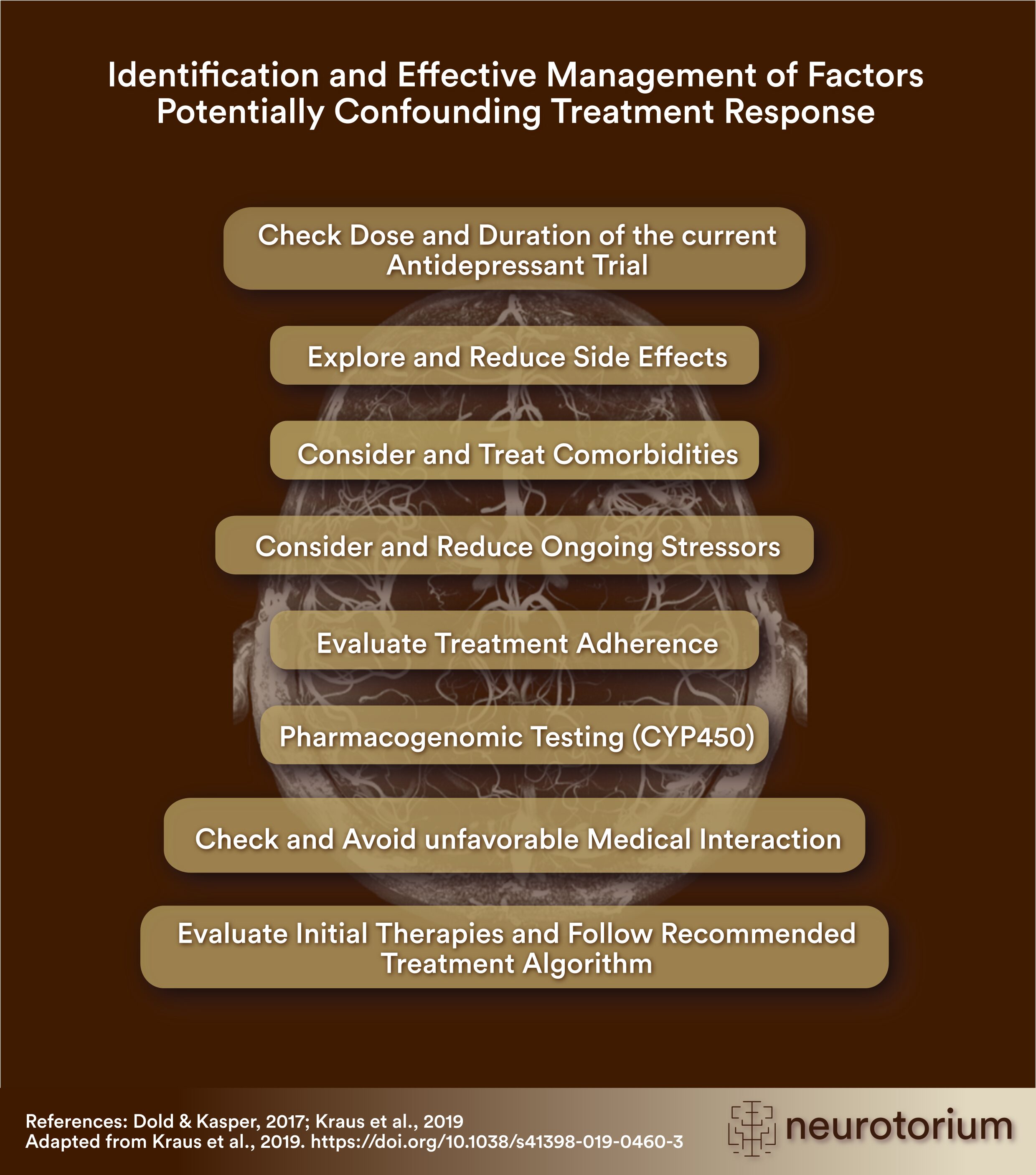
Figure 1: Identification and Effective Managment of Factors Potentially Confounding Treatment Response
There may be several factors that are potentially confounding the response to antidepressant treatment. Although they are frequently overlooked in the clinical routine, they can be very easily modified or even avoided when adequately considered and managed.7-9
However, before diagnosing TRD it is crucial to exclude the so-called pseudoresistance (Figure 1), going along with inadequate duration or dosing of ongoing antidepressant treatments, side effects, psychosocial stressors and comorbidities, as well as pharmacogenetic abnormalities leading to rapid- or poor metabolization status, incorrect diagnosis or insufficient/inadequate treatment concept.7 This is essential and should be performed as a first-step in case of insufficient response, since it has repeatedly been confirmed that an adequate consideration of pseudoresistance may avoid the development of chronicity and treatment resistance in the majority of MDD patients.1,2,7 Hence, in addition to the concept of TRD, the definition of the so-called difficult-to-treat depression (DTD) has been introduced, reflecting a broader spectrum of such common clinical and neurobiological constellations.3,8
In addition to the concept of TRD, the definition of the so-called difficult-to-treat depression (DTD) has been introduced, reflecting a broader spectrum of such common clinical and neurobiological constellations.3,8
Treatment Strategies for TRD
Given its complex etiology, TRD requires a multimodal treatment approach, incorporating pharmacological, neurostimulation-, psychotherapeutic, as well as chronobiological interventions.1,3,6,8-10 Hereby, psychopharmacotherapy has been repeatedly conformed to represent its basis and first-line treatment for MDD that might be extended by further effective add-on strategies due to the individual patient profiles including leading symptomatology, potential comorbidities and already established treatments.6,9 This is supported by available international evidence investigating the impact of patients´ treatment preferences on their outcomes that showed superior efficacy of antidepressant medication over psychotherapy in patients without any specific treatment preferences, highlighting the importance of understanding the neurobiological underpinnings of depression and its treatment, especially in cases of chronicity and TRD.11-13 Furthermore, understanding medication as an essential fundament of the individual treatment concept reflects an important analogy to other medical diseases such as hypertension or diabetes, for instance, which similarly represent multifactorial and systemic diseases resulting from the constant and dynamic interplay of genetic vulnerability and environmental factors.14 Accordingly, treatment strategies that were carefully selected according to the recommendations of current international guidelines for the diagnostics and treatment of MDD and the individual patient profiles are related to a very good prognosis even in TRD, when administered and monitored adequately.6,7,10,11,15,16
Treatment strategies that were carefully selected according to the recommendations of current international guidelines for the diagnostics and treatment of MDD and the individual patient profiles are related to a very good prognosis even in TRD.
Recommended Psychopharmacotherapy
1. Optimizing Antidepressant Psychopharmacotherapy
In the course of an evidence based first-line antidepressant treatment, the initial antidepressant agent should be selected based on the individual patient profiles (e.g., SSRIs or SNRIs in case of depressed symptoms with comorbid anxiety and psychosomatic phenomena; mirtazapine in case of depressive symptoms with predominant sleep disturbances and appetite and weight loss; bupropion in case of depressive symptoms with predominant anhedonia and reduced drive; vortioxetine in case of depressive symptoms with leading cognitive impairment) and administered in an adequate daily dose, that should be optimized gradually due to the individual tolerability and efficacy in the course of 2-4 weeks after treatment initiation).15 In cases of partial response, augmentation and combination treatment strategies are recommended due to available international evidence, while dose escalation and switching options are deemed inferior and justified only for specific clinical constellations (e.g., switching in case of absolute nonresponse or non-tolerable side effects, and dose escalation in cases of confirmed ultra-rapid metabolization status). It is therefore highly advisable to follow current treatment guidelines, which are grounded on its basis and regularly updated accordingly (Figure 2;1,7,8,15).
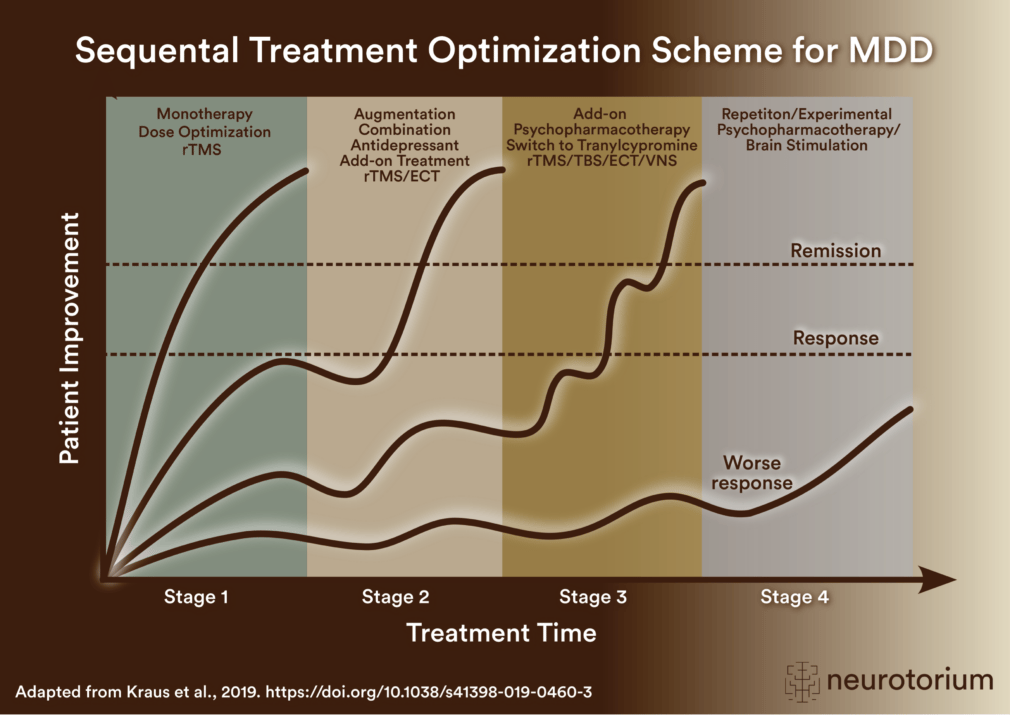
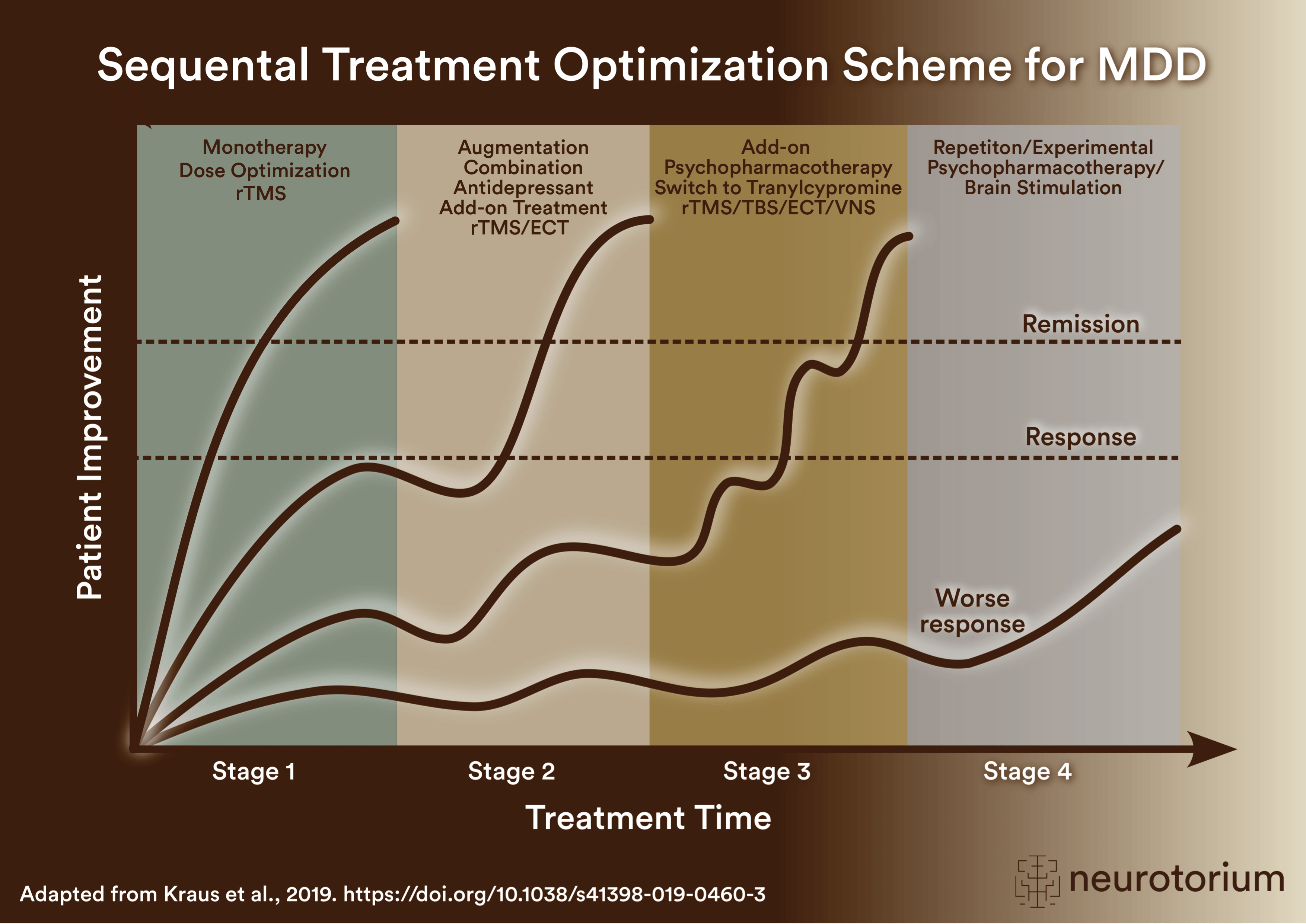
Figure 2: Sequental Treatment Optimization Scheme for Major Depressive Disorder
Sequential treatment optimization scheme for major depressive disorder generated according to international evidence.7,8 Treatment optimization steps are recommended for patients being treated for the first time (stage 1: e.g., SSRIs, SNRIs, mirtazapine, bupropion, trazodone, vortioxetine) as well as for patients with insufficient response to first- or second-stage therapies (stages 2-4). Treatment response curves are displayed for four common types of patients, underlining the importance of sequentially introducing the next step upon non-response to previous steps. Currently available treatments should be carefully selected due to the individual patient profiles, including predominant depressive symptoms and comorbidities. Despite the heterogeneity of current classifications, patients classified with TRD are eligible for the suggested second- or third-stage therapies.
Abbreviations: ECT: Electroconvulsive Therapy; rTMS: Repetitive Transcranial Magnetic Stimulation; TBS: theta-burst stimulation; VNS: Vagus Nerve Stimulation.
2. Augmentation Strategies
- Second Generation Antipsychotics (SGAs): Especially aripiprazole, brexpiprazole, cariprazine, and quetiapine have shown efficacy in TRD when used as augmentation agents, especially in patients with additional psychotic features.15 Lower daily doses as in treatment of psychotic diseases are frequently sufficient to achieve sufficient response, e.g. aripiprazole 2,5-5 mg or quetiapine 50-200 mg.8,15
- Lithium: Well-documented efficacy, particularly in reducing suicidality as well as in patients with bipolarity.15 According to current international guidelines, lithium plasma levels between 0,6-0,8 mmol/l and 0,5 mmol/l in the elderly have been shown to be effective in the course of antidepressant augmentation treatment.8,15
- Glutamatergic Agents: Intranasal esketamine is an FDA- and EMA approved add-on treatment for TRD, enabling rapid and robust symptom relief.1,15
3. Combination Strategies
- Preferably 2 antidepressants with different modes of action: e. g.,
- Selective serotonin reuptake inhibitors (SSRIs) or serotonin-norepinephrine reuptake inhibitors (SNRIs) or vortioxetine in combination with mirtazapine or trazodone, respectively.1,15
- SSRIs or Vortioxetine and bupropion1,15
- Bupropion and trazodone1,15
According to the most recent CANMAT guidelines, combinations of antidepressants are considered second-line strategies, as the evidence is less consistent compared to adjunctive treatments with SGAs or lithium, but still clinically meaningful in selected patients.8 Combination therapy can be particularly useful in patients with partial response to monotherapy, when augmentation with SGAs or lithium is not suitable or not sufficient.8 While combination strategies may provide incremental benefits in TRD, they should be applied thoughtfully, with careful attention to pharmacokinetic and safety profiles. Their clinical utility is strongest when tailored to the individual symptom profile and comorbidities.8
Accordingly, SSRIs, SNRIs, or vortioxetine will benefit from a combination with mirtazapine especially in patients with residual insomnia or appetite loss.8 Their combination with trazodone may have positive impact on potential sexual deficits, which occur commonly as a side effect of SSRIs and SNRIs. Furthermore, patients with persistent anhedonia, low energy, or cognitive impairment may benefit from the combination of SSRIs or vortioxetine with bupropion.8 The antidepressant combination of bupropion and trazodone may be very helpful in patients with prominent sleep and energy-related symptoms.8
According to the most recent CANMAT guidelines, combinations of antidepressants are considered second-line strategies, as the evidence is less consistent compared to adjunctive treatments with SGAs or lithium, but still clinically meaningful in selected patients.8
4. Experimental Psychopharmacotherapeutics
- GABAergic Modulators: Brexanolone, approved for postpartum depression, and related agents (e.g. zuranolone) are under investigation for broader depressive conditions.1,15,17 Generally, these agents are very promising but still experimental for MDD and TRD, emphasizing the need for further phase III evidence before broader clinical implementation.8
- Psychedelics (e.g. psilocybin): Emerging evidence suggests potential antidepressant effects via neuroplasticity and serotonin receptor modulation that, importantly, need to be further investigated.1,15 In line with the most recent recommendations, psychedelics are to be considered investigational, and their use is currently recommended only within the framework of clinical trials, given limited evidence and regulatory considerations.8
- Anti-Inflammatory Agents: TNF-α inhibitors and IL-6 antagonists are being explored as adjunctive treatments.1,15 Although initial findings are encouraging, these agents remain experimental, requiring more robust and reproducible evidence before recommendation in routine TRD management.8
Neurostimulation Therapies
- Electroconvulsive Therapy (ECT): Remains the most effective treatment for severe and psychotic depression as well as the gold-standard treatment for TRD.1,10,15,16 Besides its superior efficacy across acute, psychotic, and treatment-resistant presentations, careful patient selection and consideration of maintenance strategies to prevent relapse are important.8
- Repetitive Transcranial Magnetic Stimulation (rTMS): FDA-approved for TRD; theta-burst stimulation (TBS) may enhance efficacy.1,8,10,15
- Vagus Nerve Stimulation (VNS): Approved for chronic TRD but with variable efficacy, that is mostly pronounced in longer term.1,15,18 VNS may be considered in highly treatment-resistant cases, where conventional interventions, including ECT and rTMS, have been insufficient.8
- Deep Brain Stimulation (DBS): Investigational therapy targeting specific neural circuits involved in mood regulation for TRD patients who have not responded to rTMS, ECT and VNS.1,8,15
Psychotherapeutic and further Adjunctive Interventions
- Cognitive Behavioral Therapy (CBT): Effective as an adjunct to psychopharmacotherapy,1,11,12,15 especially when sequentially used following response to acute-phase psychopharmacotherapy.19 CBT is considered a first-line adjunctive strategy for TRD, as it not only improves symptomatic outcomes but also enhances functional recovery and reduces relapse risk. Other evidence-based psychotherapies, such as interpersonal therapy (IPT) or mindfulness-based cognitive therapy (MBCT), may also be considered in selected patients.8
- Chronotherapeutic Strategies: Bright light therapy and sleep deprivation have shown promise in modulating circadian rhythms and might, hence, be effective as an adjunct to pharmacotherapy, especially in patients with seasonal patterns as well as atypical clinical manifestations and bipolarity.1,15,20
Importantly, the abovementioned non-pharmacological interventions might represent very effective supportive options, best applied in combination with ongoing pharmacological treatment rather than as stand-alone strategies.8
Future Directions
Advancements in precision psychiatry, including pharmacogenomics and biomarker-driven treatment selection, hold promise for improving TRD outcomes.1,10 Especially, the integration of pharmacogenetic testing may support individualized treatment choices in specific cases.8 Digital therapeutics and artificial intelligence-driven treatment algorithms are also emerging as innovative approaches,21 potentially supporting clinical decision-making and enhancing adherence.8 Furthermore, the recently introduced concept of DTD expands the framework beyond TRD by capturing broader and more heterogeneous clinical constellations, underscoring the importance of functional outcomes, collaborative care, and long-term management strategies.8
Digital therapeutics and artificial intelligence-driven treatment algorithms are also emerging as innovative approaches, 21 potentially supporting clinical decision-making and enhancing adherence.8
Conclusion
TRD remains a significant clinical challenge, necessitating individualized, evidence-based treatment strategies.1,2,5-11,16,17 While conventional psychopharmacotherapy remains the mainstay, novel interventions targeting glutamatergic, GABAergic, and inflammatory pathways are expanding treatment options.10,16 Integrating multimodal approaches and leveraging emerging technologies will be critical in optimizing outcomes for patients with TRD.1,2,5-11,16,17
It is of utmost importance to emphasize that major depressive episodes, that are treated according to available evidence-based recommendations, are related to a very good prognosis.7,8 This is clinically very relevant, since a considerable number of patients with MDD has repeatedly been shown to receive inadequate treatments.8,11 Hence, the so-called pseudoresistance, representing a very frequent and, importantly, avoidable clinical phenomenon, should be excluded in first instance in case of non-response.8 Finally, the psychoeducational and motivational support towards positive mental health and general well-being of the affected patients, which is performed during the regular rounds at psychiatric hospitals and/or consultations at outpatient units, represents a very effective intervention significantly contributing to the overall beneficial effects together with ongoing psychopharmacotherapy and/or other modality of the broad armamentarium of available treatment strategies.1,2,5-11,16,17
It is of utmost importance to emphasize that major depressive episodes, that are treated according to available evidence-based recommendations, are related to a very good prognosis.7,8
Related content
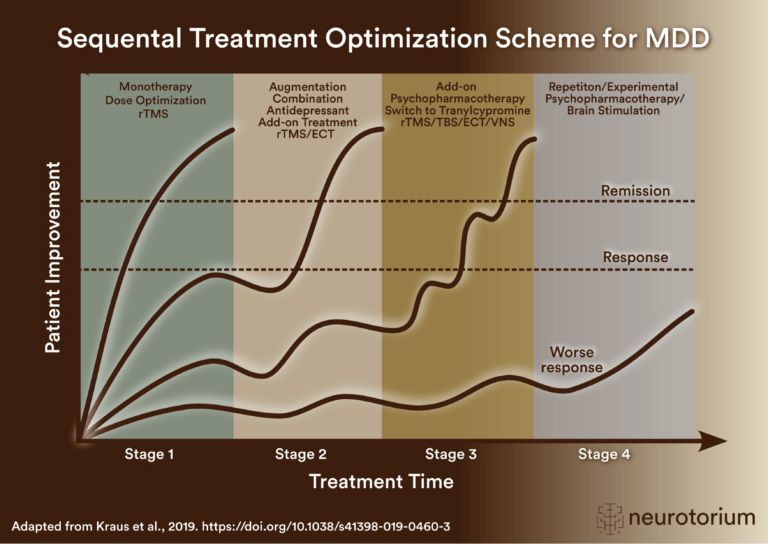
Sequential treatment optimization scheme for major depressive disorder generated according to international evidence.

Key steps for managing factors that may confound antidepressant treatment response, including dose, side effects, comorbidities, stressors, adherence, pharmacogenomics, interactions, and treatment algorithms.
{kind=link}
{kind=link}