


For millions struggling with mental illness, and for their healthcare providers, the path to effective treatments remains a frustrating journey of trial and error. Treatment resistance, defined as a lack of response to conventional treatment paradigms, affects 20–60% of patients across psychiatric disorders1 and has a substantial personal and societal impact. Traditional first-line antidepressants, for example, lead to remission of depressive symptoms in only 30% of patients2, leaving many without relief. Yet psychiatric research has underinvested in understanding why well-established treatments fail to help such a large number of patients.
The idea that psychiatric diagnoses reflect single, uniform diseases has been questioned since the introduction of the DSM (Diagnostic and Statistical Manual of Mental Disorders) in 1952 and the inclusion of a mental health chapter in ICD-6 (International Classification of Diseases) in 1949. Despite scientific progress, the most recent editions (DSM-5-TR, 2022 and ICD-11, 2022) of both diagnostic frameworks still do not account for the biological heterogeneity within diagnostic categories. These symptom-based frameworks remain the standard in clinical practice, guiding not only treatment decisions, but also insurance policies, as well as drug development and approval processes. If we want to bring change, we have to move beyond this diagnostic framework and recognize that current diagnostic classifications may group together biologically and mechanistically distinct subtypes of patients. Having a fever is a useful analogy: like depression, it is also a common clinical presentation of many underlying processes, ranging from infections to cancer. And while fever often responds to antipyretics, it is the underlying cause that ultimately determines the most appropriate treatment. This applies to depression as well: the breakthroughs won’t come from applying the same treatment algorithm to everyone who meets the criteria of a DSM or ICD code, but from implementing more effective, personalised, and biologically informed regimens: the right treatment for the right patient at the right time3.
A growing body of evidence now supports this concept of precision psychiatry, where treatment is tailored to an individual’s biological and clinical profile rather than to symptom-based diagnoses. This article presents the potential of targeted therapies to provide more effective, personalised treatment options, and the leading role of immunopsychiatry within precision psychiatry.
If we want to bring change, we have to move beyond this diagnostic framework and recognize that current diagnostic classifications may group together biologically and mechanistically distinct subtypes of patients.

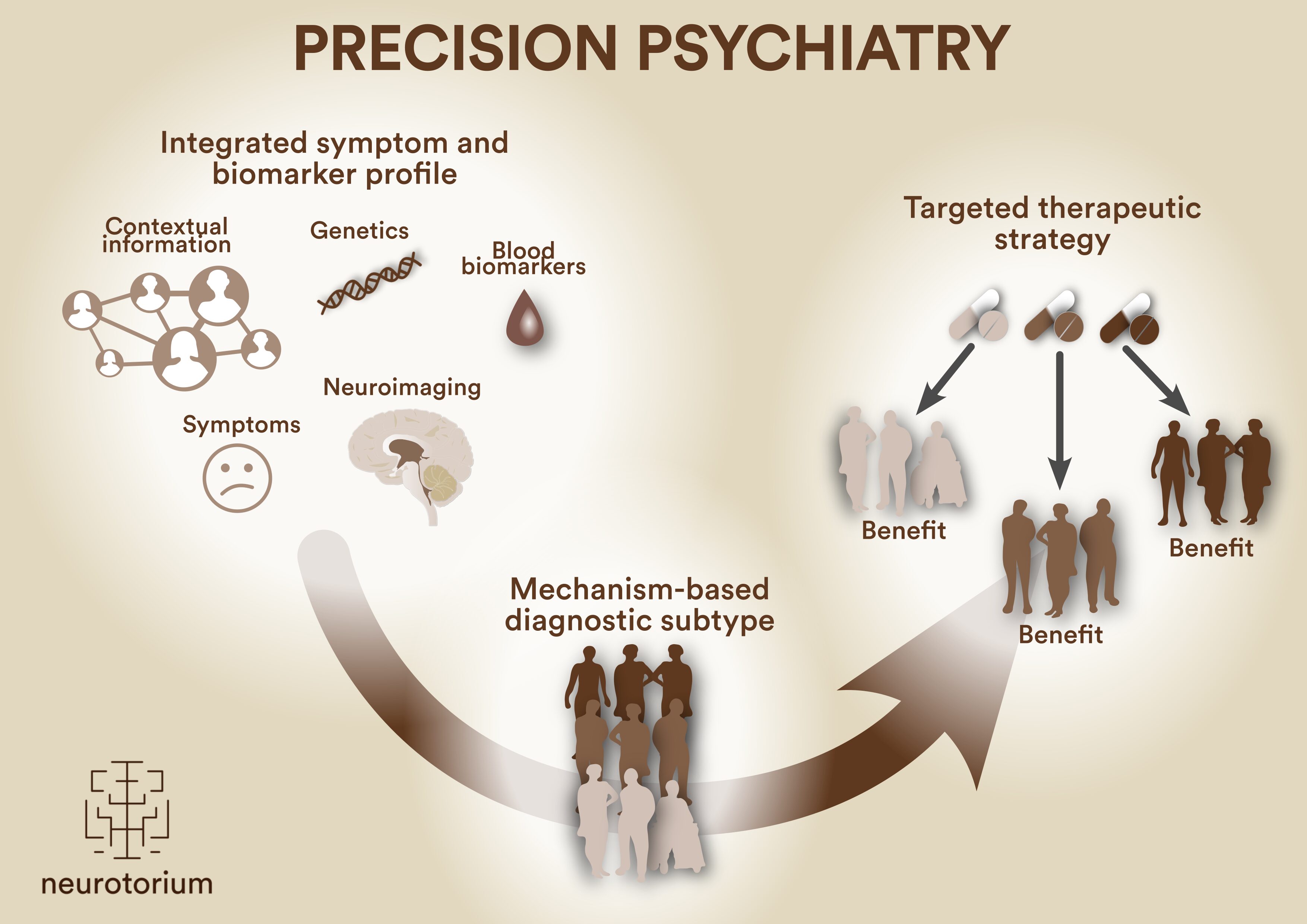
Figure 1: Mechanism-based subtyping to inform targeted therapies
Precision psychiatry aims to move beyond traditional symptom-based diagnostic frameworks which group biologically heterogeneous patients under the same diagnosis. By integrating contextual information, genetic data, blood biomarkers, symptom profiles and neuroimaging findings, patients can be stratified into mechanism-based subtypes. This stratification enables the identification of targeted therapeutic strategies matched to the underlying biological mechanisms. This can improve treatment efficacy and reduce the current trial-and-error approach.
A growing global movement towards precision psychiatry
Precision psychiatry is no longer a futuristic ideal: it is steadily progressing toward clinical implementation, supported by major international initiatives that aim to develop the necessary tools, frameworks, and policies. The ECNP (European College of Neuropsychopharmacology), for example, has developed a multi-stakeholder Roadmap for Precision Psychiatry and is leading collaborative efforts to integrate biology into psychiatric diagnostics and treatment. Their recent position paper4 underscores the urgency of moving beyond symptom-based classifications toward biologically informed patient stratification. In parallel, the Global Summits on Precision Psychiatry, hosted by Fondation FondaMental, has called for a broad vision of precision psychiatry3: not limited to biomarker discovery, but also policy change, regulatory support, clinician training, and the development of multidisciplinary expert centers. These international efforts signal a shared commitment: to reshape psychiatry into a field guided by mechanism-based, personalised care.
Immunopsychiatry taking the lead in precision psychiatry
Although precision psychiatry is not yet standard in daily practice, immunopsychiatry is among the most advanced in its translation into clinical implementation, largely driven by the inherently transdiagnostic nature of immune-based mechanisms in psychiatric disorders.
A large body of evidence suggests that for certain patients, inflammation is a major driver of psychiatric symptoms5 and a predictor of poor response to traditional treatments6, regardless of the psychiatric diagnosis7. This insight is shifting the treatment paradigm toward interventions that are tailored not just to symptoms but to this underlying immunological mechanism driving them8. One of the most illustrating examples is the recognition of CNS (central nervous system) and systemic autoimmunity as a treatable cause and/or contributing factor for several psychiatric presentations, including those similar to psychotic disorders, depression, or OCD (obsessive-compulsive disorder) without overt neurological symptoms. Clinical guidelines now recommend screening for blood and cerebrospinal fluid autoantibodies in atypical or severe treatment-resistant cases, and the term autoimmune psychosis is increasingly accepted in the field9,10.
While pure autoimmune conditions likely make up only a small fraction of all psychiatric presentations, immune system involvement is not limited to these rare conditions. A much larger proportion may present with comorbidity between psychiatric disorders and various (sometimes undiagnosed) autoimmune conditions (such as rheumatoid arthritis, systemic lupus erythematosus, inflammatory bowel conditions or psoriasis), with both conditions influencing each other. Furthermore, large biobank studies show that approximately 27% of depressed patients demonstrate some degree of low-grade inflammation11. Individuals exposed to childhood maltreatment or early life infections may be particularly primed for immune abnormalities, which are observed across DSM diagnostic categories12. This invites us to think of immune-mediated mental illness as a dimensional and transdiagnostic continuum: from rare, autoimmune presentations to somatic-psychiatric comorbidity and to common psychiatric pathophysiology modulated by low-grade inflammation13.
Clinical guidelines now recommend screening for blood and cerebrospinal fluid autoantibodies in atypical or severe treatment-resistant cases, and the term autoimmune psychosis is increasingly accepted in the field9,10.
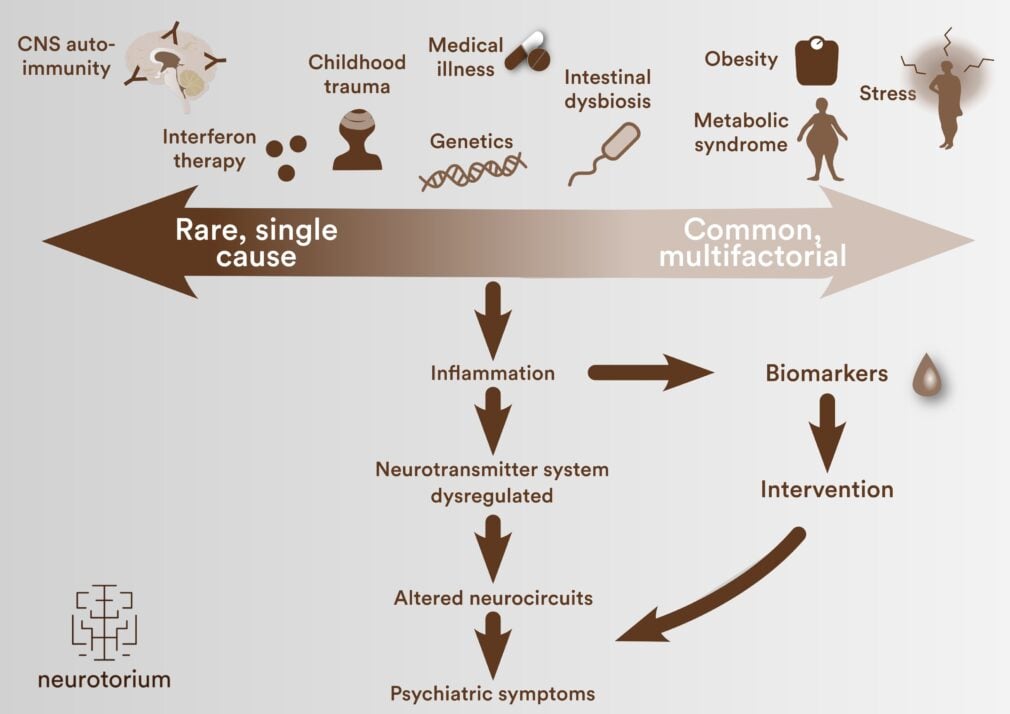
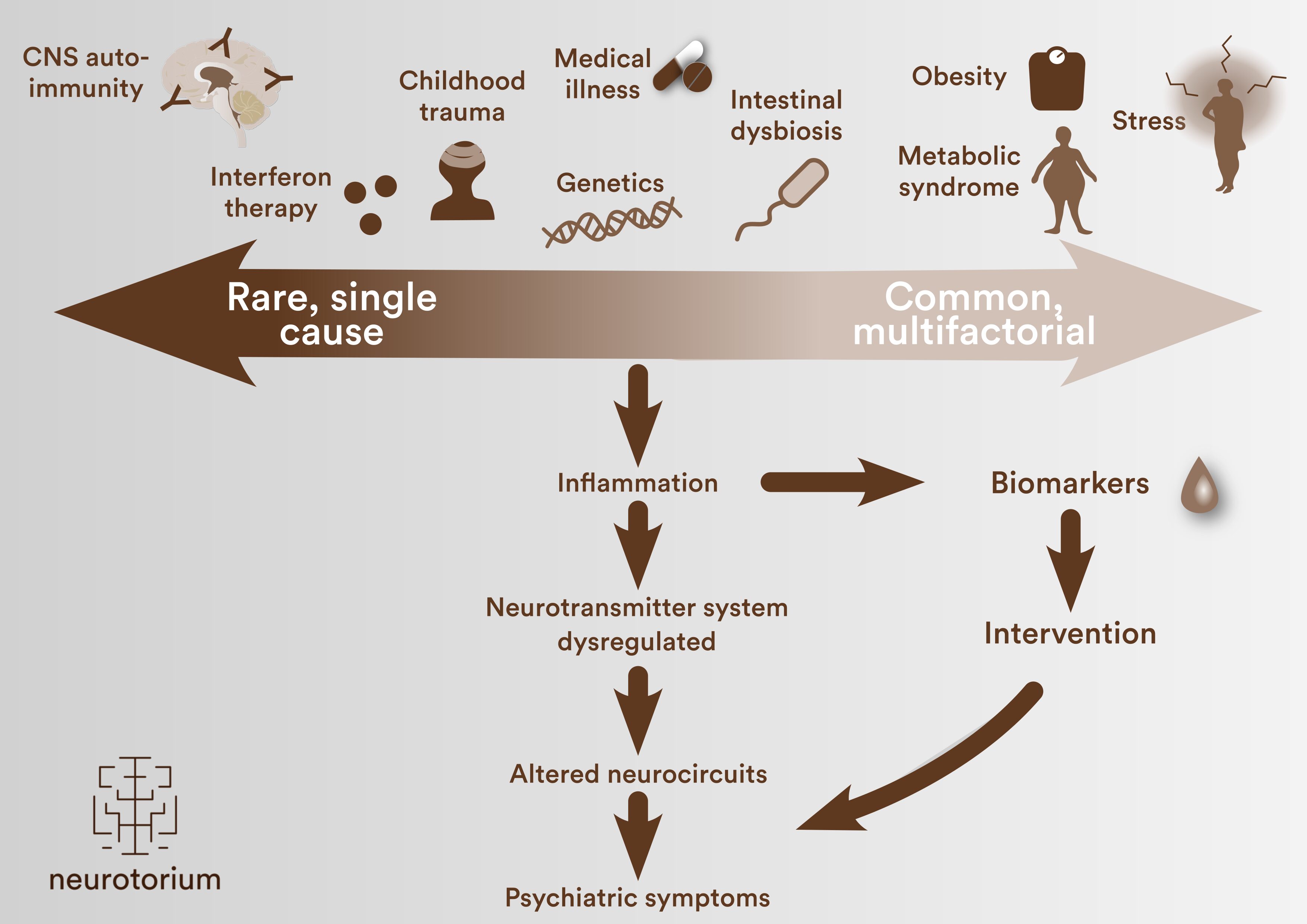
Figure 2: The immunopsychiatry continuum
On the continuum of immune-mediated mechanisms contributing to psychiatric symptoms, the relative contribution of immune activation differs across patient groups. At one end (left), rare single-cause processes such as interferon therapy-induced neuropsychiatric effects (e.g. in hepatitis C treatment) act as direct triggers. At the other end (right), common and often multifactorial factors, including obesity, metabolic syndrome, stress and genetic vulnerability, indirectly promote immune dysregulation. Regardless of the initiating cause, inflammation can lead to neurotransmitter system dysregulation and altered neurocircuits, resulting in psychiatric symptoms. Biomarker assessments can help identify these immune-mediated processes and inform targeted intervention strategies.
How inflammation leads to depression
When the immune system is activated, the body initiates a set of physiological responses known as sickness behavior, triggered by pro-inflammatory cytokines such as interleukin-6 (Il-6) and C-reactive protein (CRP). Most people know how this feels from the early stages of infections like the flu: feeling disproportionately tired, unmotivated, lethargic, uninterested in social or rewarding activities, and mentally foggy. This behavior is evolutionarily adaptive, as it helps the body conserve energy, prioritizes fighting the virus and avoids spreading it14.
However, when immune activation becomes persistent, as reflected in chronically elevated immune markers, this response is no longer protective. Instead, it can disrupt the hypothalamic-pituitary-adrenal (HPA) axis, reinforce a pro-inflammatory state15, and affect brain circuits involved in motivation, reward, and cognition, including the prefrontal cortex, hippocampus, and striatum. It also interferes with neurotransmitter systems leading to the continuation of sickness behavior symptoms such as motivational anhedonia and fatigue16. Understanding these psychiatric symptoms as consequences of systemic immune activation could redefine both diagnosis and treatment in psychiatry13.
Important research suggests that persistent immune activation may not only trigger symptoms but also impair the brain’s ability to recover from a psychological decompensation through reduced brain plasticity17-19. This so-called “inflammatory trap” may help explain why some individuals remain stuck in a depressive state despite appropriate treatment. Calming down the immune system may help restore the brain’s capacity to adapt and change. In this light, precision psychiatry is not just about what treatment to give, but also when the brain is biologically ready to benefit from it. Once again: the right treatment for the right patient at the right time3.
This so-called “inflammatory trap” may help explain why some individuals remain stuck in a depressive state despite appropriate treatment.
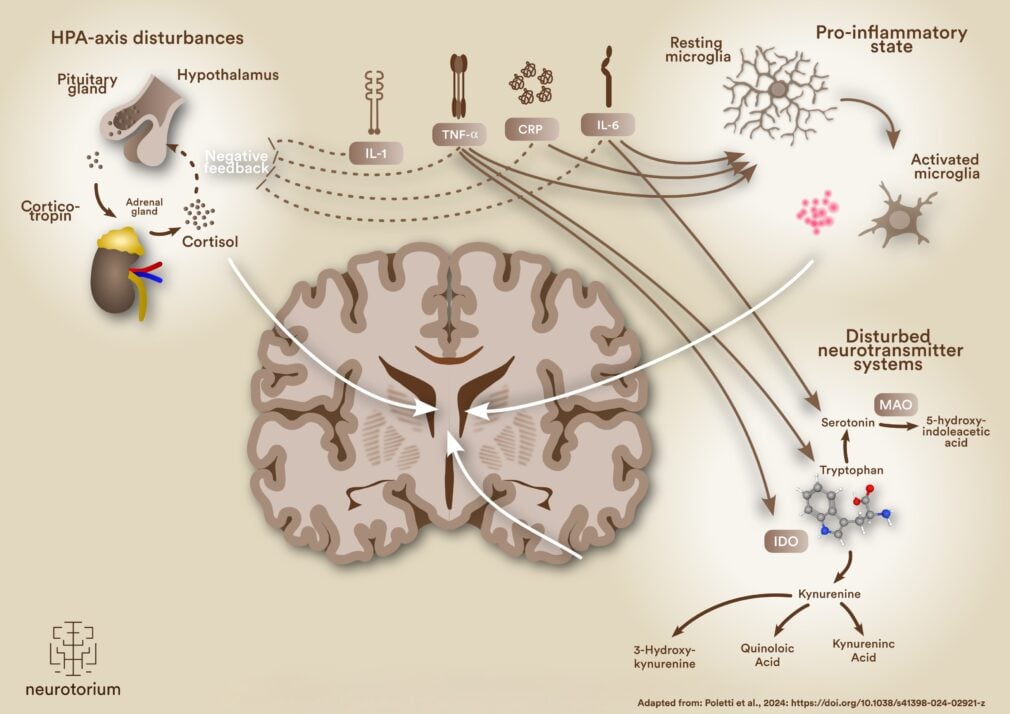
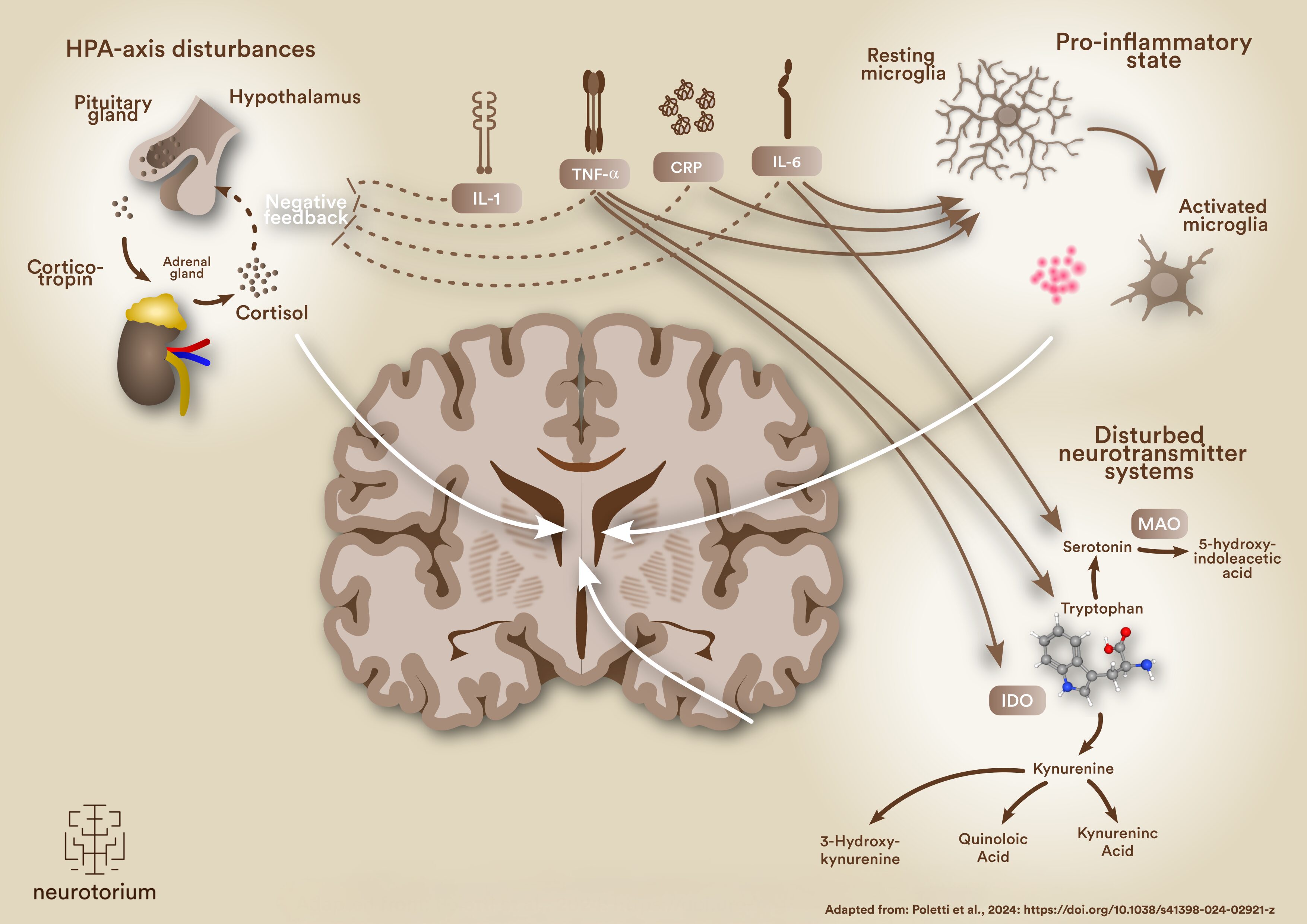
Figure 3: Chronic immune activation disrupts brain circuits and neurotransmission
Acute immune activation triggers adaptive sickness behaviour through the release of pro-inflammatory cytokines, such as interleukin-1 and -6 (IL-1 and -6), tumor necrosis factor-α (TNF-α) and C-reactive protein (CRP). When the immune system is persistently activated, these disrupt normal feedback in the hypothalamic-pituitary-adrenal (HPA) axis (top left), leading to sustained cortisol release. Simultaneously, microglial cells in the brain shift from a resting to an activated state (top right). These disturbances contribute to a pro-inflammatory state that impairs brain regions involved in motivation, reward and cognition. Dysregulation of other pathways such as the tryptophan–kynurenine pathway (bottom right) further contributes to neurotransmitter imbalances, reducing serotonin availability and promoting neurotoxic metabolites.
Identifying and treating immune-mediated depressions
Rebalancing the immune system is not necessarily difficult: several anti-inflammatory medications are already available for a long time. The real question is for which psychiatric patients, beyond those with clear autoimmune cases, this is an appropriate therapeutic option. In depression, for example, more than 18 placebo-controlled trials of a range of immune-targeted pharmacological interventions have found small-to-moderate effect sizes for improving depressive symptoms when added to treatment as usual 6,20,21. Yet despite these encouraging findings, translation to clinical practice remains limited. Even for celecoxib and minocycline, two of the most promising agents, results have been inconsistent across studies22,23. Two issues stand in the way: the difficulty of identifying the right patients, and of measuring the treatment effect3,13.
First, many existing studies have failed to effectively include patients based on inflammatory status. Post hoc analyses of three studies have shown that the antidepressant efficacy of anti-inflammatories was limited to patients with elevated inflammation, specifically those with high-sensitivity C-reactive protein (hsCRP) levels above 3 mg/L (minocycline and N-acetylcysteine)24,25 and above 5mg/L (infliximab). Similarly, post hoc analysis of statins in schizophrenia spectrum disorders revealed that only patients in the inflammatory subgroup showed a consistent reduction in symptom severity over time26.
Two issues stand in the way: the difficulty of identifying the right patients, and of measuring the treatment effect3,13.
Complicating matters further, traditional standardized outcome measures for depression, like the HAM-D or MADRS, do not measure symptoms linked to inflammation, such as motivational anhedonia, hypersomnia, hyperphagia, or leaden paralysis27. Together with the exclusion of patients with comorbid inflammatory disorders, this leads to underrepresentation or exclusion of patients who may benefit most, simply because they do not meet the inclusion thresholds on these traditional rating scales. And consequently, potential treatment effects may not be accurately captured either.
Both of these issues highlight the importance of selectively enriching or stratifying clinical trials for patients in the target population by using baseline measurements of inflammatory biomarkers, as well as choosing or developing more appropriate outcome measures to accurately capture the treatment effect.
To overcome these obstacles, major international initiatives are now stepping in. The Belgian INSTA-MD trial28 is a prospective study testing anti-inflammatory treatments in patients with depression, specifically enriching the study population with participants who have elevated CRP levels. Similarly, the Dutch INFLAMED study29 focuses on participants with both immune and metabolic disturbances, assessing the potential of anti-inflammatory medication in this subgroup. The ASPIRE study, funded by the Wellcome Trust, takes a retrospective approach by pooling data from previous clinical trials of anti-inflammatories in depression. It’s a large international collaboration involving many leading (immunopsychiatry) researchers and aims to develop a biomarker-driven decision tool to guide the clinical use of anti-inflammatory treatments. True to the principle of nothing about us without us, it is co-led by people with lived experience to ensure socially responsible and clinically relevant outcomes.
Together, they aim to answer the central question in immunopsychiatry: in whom, when, and how should we influence the immune system to restore mental health?
Complicating matters further, traditional standardized outcome measures for depression, like the HAM-D or MADRS, do not measure symptoms linked to inflammation, such as motivational anhedonia, hypersomnia, hyperphagia, or leaden paralysis27.
Future directions
The future of psychiatric practice lies in more precise, biologically grounded approaches. Within the context of precision psychiatry, this means shifting from a classification-based toward mechanism-based precision approach. Moving forward, precision psychiatry research will increasingly focus on clinical- and biomarker-driven patient selection, enabling clinicians to identify those who are most likely to benefit from specific targeted therapies, improving treatment outcomes and reducing unnecessary side effects.
Immunopsychiatry is taking a leading role in this evolution, because this discipline is both fundamentally transdiagnostic and mechanism-based in nature: across DSM categories, a substantial subset of patients appears to fall within the spectrum of immune-mediated psychiatric illness. However, to fully realize its potential, researchers, industry, and regulators will have to adopt innovative trial designs and let go of DSM-based patient selection and outcome measures.
Ultimately, integrating precision psychiatry and immunopsychiatry approaches into clinical practice has the potential to transform psychiatric treatments. This approach offers hope for those who have not responded to conventional treatments. We’re getting closer and closer to a future where psychiatric illnesses are not one-size-fits-all conditions, but heterogeneous disorders addressed through mechanism-based interventions.
Within the context of precision psychiatry, this means shifting from a classification-based toward mechanism-based precision approach.
Related content
Treatment-resistant depression (TRD) represents a significant clinical challenge, affecting approximately 30% of individuals with major depressive disorder (MDD) who fail to respond to at least two adequate antidepressant trials.
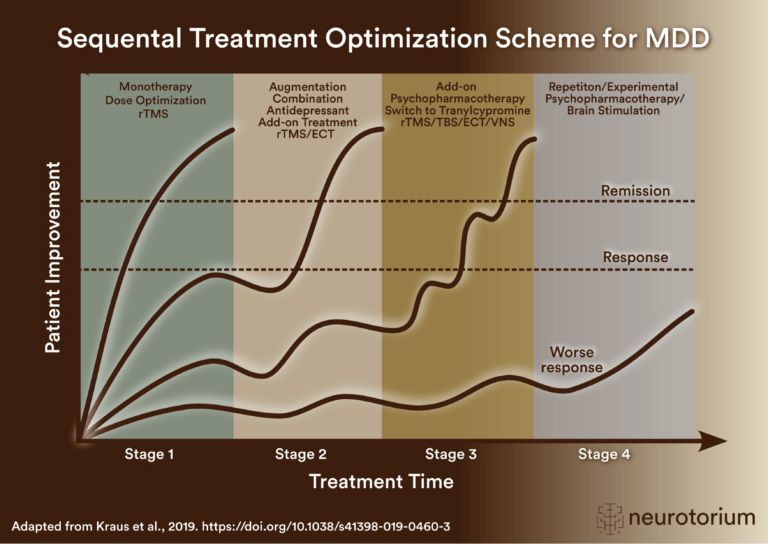
Sequential treatment optimization scheme for major depressive disorder generated according to international evidence.

{kind=link}
{kind=link}
{kind=link}
Key steps for managing factors that may confound antidepressant treatment response, including dose, side effects, comorbidities, stressors, adherence, pharmacogenomics, interactions, and treatment algorithms.