
Migraine Impact and Treatment
Migraine is a disabling and prevalent neurological disorder that affects approximately one billion people worldwide.1 It is the world’s second leading cause of disability, accounting for more years lived with disability than all other neurological disorders combined2 (Figure 1). Migraine is characterized by recurrent attacks of moderate to severe headache, often accompanied by hypersensitivity to light and sound, as well as nausea and vomiting.3 These attacks can last from hours to several days, significantly impairing daily activities and quality of life. About a third of individuals with migraine also experience aura—fully reversible and transient neurological symptoms that commonly manifest as visual disturbances preceding the onset of headache.4
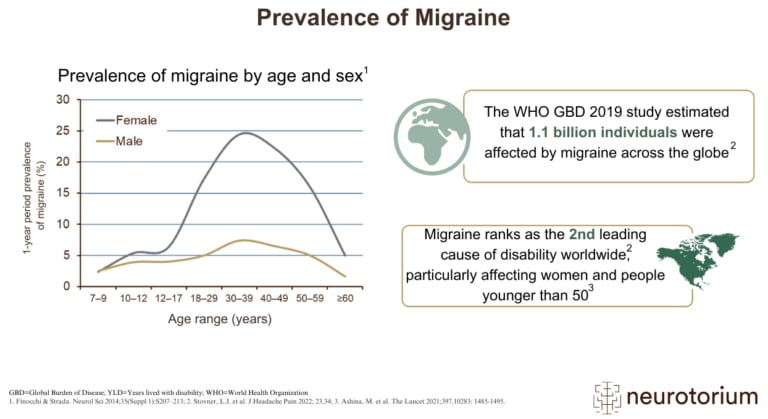
It is the world’s second leading cause of disability, accounting for more years lived with disability than all other neurological disorders combined2

Figure 1. Prevalence of Migraine
Migraine affects an estimated 1.1 billion people worldwide and ranks as the 2nd leading cause of disability, while being the leading among young adults.1,31,32 There is a female predominance of approximately 2:1, and the prevalence surges throughout puberty, peaks around age forty, and finally declines in the elderly. Migraine without aura is the most common form, whereas a third experience attacks of migraine with aura either exclusively or in addition to attacks without aura.
Historically, the management of migraine has been underprioritized, with few dedicated treatments available. A significant breakthrough occurred in the 1990s with the development of triptans, which are serotonergic agonists targeting 5-HT1B/1D receptors used in the acute treatment of migraine attacks.5 Triptans were designed to mimic the serotonergic effects of ergot alkaloids, providing high efficacy in treating individual migraine attacks while minimizing the risk of serious side effects associated with ergots. The success of triptans shifted the focus from treating individual attacks to preventing future ones, emphasizing the need for effective preventive treatments. Another rationale for preventive therapy was the observation that frequent use of acute treatments could paradoxically increase headache frequency, a phenomenon known as medication-overuse headache.6 Despite the availability of some non-specific preventive medications, they often had limited efficacy or considerable side effects, highlighting the need for more effective options.7
Human Models of Migraine
To advance understanding of migraine pathophysiology and develop effective treatments, human experimental models of migraine have been invaluable.8 These models involve inducing migraine-like attacks in susceptible individuals under controlled conditions, allowing researchers to study underlying mechanisms and test potential therapeutic agents. Substances known to provoke migraine attacks, such as nitroglycerin,9 calcitonin gene-related peptide (CGRP),10 and pituitary adenylate cyclase-activating polypeptide-38 (PACAP-38),11 have been used in these models. In these models, an individual with migraine receives a suspected migraine-triggering substance either orally or by infusion (Figure 2). Subsequently, the headache response and intensity are systematically recorded at preset intervals. As a control, the same participant receives a placebo on a separate day, typically within a randomized, double-blinded, two-way crossover design. This methodology enables investigators to characterize the temporal development of headache and migraine in response to a suspected trigger.
These models involve inducing migraine-like attacks in susceptible individuals under controlled conditions, allowing researchers to study underlying mechanisms and test potential therapeutic agents

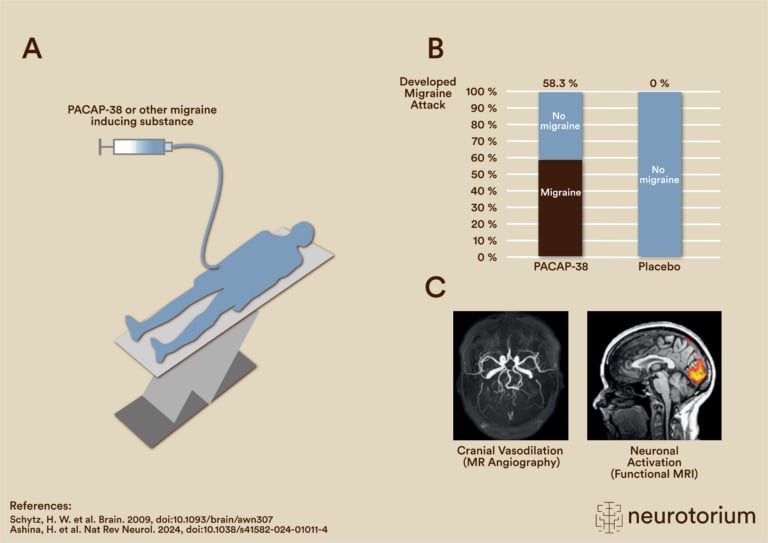
Figure 2: Human models of migraine
In human models of migraine, a suspected pharmacological migraine trigger is administered either orally or via infusion to a participant with migraine or a healthy volunteer, typically within a double-blind, randomized, placebo-controlled design.8 This allows for the identification of molecules involved in the generation of migraine attacks, and thereby reveals potential treatment targets. Moreover, migraine attacks can be reliably induced to investigate their pathophysiological underpinnings using e.g. advanced magnetic resonance imaging to investigate vasodilation or changes in neuronal activity.
MRI = Magnetic Resonance Imaging; PACAP-38 = Pituitary Adenylate Activating Polypeptide-38.
Human Models of Migraine in Treatment Development
Key insights derived from human models of migraine have led to breakthroughs in preventive migraine treatment. Investigations into the trigeminovascular system, considered the anatomical and physiological substrate of migraine headache12 (Figures 3 and 4), identified CGRP as a prominent neuropeptide involved in nociceptive signaling and vasodilation.13 Using the human migraine model, studies demonstrated that intravenous infusion of CGRP could trigger migraine attacks in individuals with migraine but not in healthy controls.10,14 This finding established CGRP as a key molecule in migraine pathogenesis and spurred extensive research into developing CGRP antagonists as potential migraine treatments. The development of gepants, small-molecule CGRP-receptor antagonists, initially faced challenges due to hepatotoxicity.15 However, the advent of monoclonal antibodies targeting CGRP or its receptor renewed interest in this therapeutic approach.13 Clinical trials demonstrated that these therapies significantly reduced migraine frequency, with about half of the treated patients experiencing at least a 50% reduction in monthly migraine days.16 This efficacy marked an unprecedented advancement in preventive migraine treatment.
This finding established CGRP as a key molecule in migraine pathogenesis and spurred extensive research into developing CGRP antagonists as potential migraine treatments

Figure 3. The Trigeminovascular System and Migraine
The trigeminovascular system is recognized as the anatomical and physiological substrate of migraine.12 Within this system, migraine-inducing and vasodilatory substances are thought to initially cause the activation of pain-sensitive first-order neurons that innervate meningeal blood vessels. The cell bodies of these neurons reside in the trigeminal ganglion, from which pain signals are transmitted unto second-order neurons of the spinal trigeminal nucleus (SpV) in the brainstem that relay to third-order neurons in the thalamus. From there, signals are sent to numerous cortical and subcortical sites to ultimately yield a migraine attack.
The initial substrate for migraine is thought to differ between attacks of migraine with and without aura. In attacks of migraine with aura, cortical spreading depolarization (the neural substrate of aura) might produce the initial stimulus for activation of first order neurons. In attacks of migraine without aura, migraine-inducing substances are thought to be released from the trigeminal system itself. Moreover, activation of the parasympathetic system from the superior salivatory nucleus (SSN) can cause the release of migraine inducing neuropeptides, such as pituitary adenylate cyclase-activating polypeptide-38 (PACAP-38), to trigger meningeal vasodilation and activation of first order neurons.
Despite the promise of CGRP-targeted therapies, limitations remained. Only about half of the patients achieved significant reductions in migraine frequency, and many continued to experience a substantial number of migraine days.17 Furthermore, in acute migraine treatment, gepants were less effective than traditional treatments like triptans.18 These challenges underscored the need for further research into alternative therapeutic targets.
Emerging Therapies for Migraine
Building upon human models of migraine, experimental studies investigated other neuropeptides involved in migraine pathophysiology. Pituitary adenylate cyclase-activating polypeptide-38 (PACAP-38), like CGRP, is expressed within the trigeminovascular system and has potent vasodilatory properties.19 Studies demonstrated that infusion of PACAP-38 induced migraine attacks in individuals with migraine but not in healthy controls.11 This finding suggested that PACAP-38 plays a significant role in migraine and could be a potential therapeutic target. Further studies explored the mechanisms involved. The combination of human migraine models with advanced magnetic resonance imaging (MRI) demonstrated that both PACAP-38 and CGRP cause dilation of the middle meningeal artery, supporting the concept that vascular changes contribute to migraine pathogenesis.20,21 Functional MRI studies indicated that PACAP-38 induced migraine attacks are associated with altered neuronal activity in pain-processing centers of the brain.22
The combination of human migraine models with advanced magnetic resonance imaging (MRI) demonstrated that both PACAP-38 and CGRP cause dilation of the middle meningeal artery
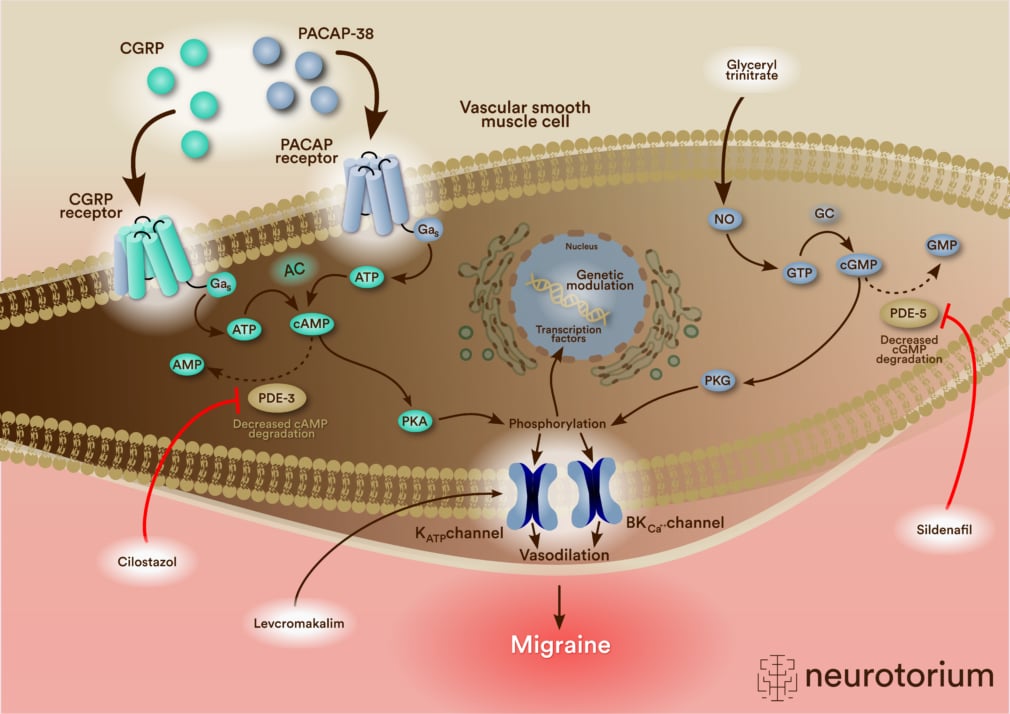
Figure 4. Vascular Signals in Migraine
Evidence from human models of migraine as well as other lines of research suggests a putative model for the genesis of migraine attacks.17 Within vascular smooth muscle cells of cephalic arteries, migraine-inducing substances act through intracellular second messengers including cyclic adenosine monophosphate (cAMP) or cyclic guanosine monophosphate (cGMP) to eventually cause the opening of ATP-sensitive potassium (KATP) channels or large-conductance Ca2+-activated K+ (BKCa) channels. This causes release of potassium from vascular smooth muscle cells and subsequently vasodilation. The efflux of potassium might activate adjacent perivascular nerve fibers to trigger the perception of migraine pain.
AMP = Adenosine Monophosphate; ATP = Adenosine Triphosphate; CGRP = Calcitonin Gene-Related Peptide; GMP = Guanosine Monophosphate; GTP = Guanosine Triphosphate; NO = Nitric Oxide; PACAP-38 = Pituitary Adenylate Cyclase-Activating Polypeptide-38; PDE-3; Phosphodiesterase-3; PDE-5; Phosphodiesterase-5; PKA = Protein Kinase A; PKG = Protein Kinase G.
Initial development efforts focused on targeting the PAC1 receptor, primarily expressed in neuronal tissues.23 However, an antibody targeting the PAC1 receptor failed to demonstrate efficacy in a phase II clinical trial,24 prompting a shift toward targeting the PACAP ligand itself. A monoclonal antibody against PACAP showed promise in a phase I trial in healthy volunteers.25 The antibody blocked vasodilation and reduced headache following PACAP-38 infusion, suggesting inhibition of vascular signals integral to migraine attack generation. A recent phase II clinical trial investigated the efficacy of the anti-PACAP antibody in preventing migraine in patients who had failed multiple prior preventive treatments and had a high frequency of monthly migraine days.26 The trial demonstrated that a single dose of the antibody significantly reduced monthly migraine days compared with placebo, offering hope for patients with refractory migraine. The reduction was comparable to that observed in trials of anti-CGRP monoclonal antibodies in the same phase.27,28
Despite these encouraging results, critical questions remain regarding PACAP’s involvement in migraine. Identifying the exact molecular mechanisms by which PACAP induces migraine attacks, including its site and receptor of action, is essential. By targeting specific receptors at precise sites, it might be possible to optimize therapeutic effects. Notably, a fourth PACAP receptor on mast cells has emerged as a potential target.29,30 Understanding shared mechanisms between PACAP and CGRP could also lay the foundation for future advances in migraine treatment.
Despite these encouraging results, critical questions remain regarding PACAP’s involvement in migraine
Migraine is a common neurological disorder affecting over 1 billion people worldwide, causing debilitating headaches often accompanied by light and sound sensitivity, nausea, and more. Despite its prevalence, the underlying causes of migraine remain incompletely understood.
In this video, Rune Häckert Christensen, MD, PhD-fellow discusses how human models of migraine have identified key molecular triggers like CGRP and PACAP, leading to a revolution in treatment. These discoveries have not only improved outcomes for many patients but also hold promise for those who don’t respond to current therapies.
Conclusion
The use of human models of migraine has been instrumental in advancing our understanding of migraine pathophysiology and in the development of novel therapies. By identifying key neuropeptides like CGRP and PACAP-38 and demonstrating their roles in inducing migraine attacks, researchers have been able to develop targeted therapies that offer significant benefits to patients. While therapies targeting the CGRP pathway have revolutionized migraine treatment, the emerging treatments targeting PACAP signaling hold promise for further advancements, particularly for patients who do not respond to existing medication. Continued research is needed to fully elucidate the mechanisms by which PACAP induces migraine and to identify the most effective therapeutic targets within its signaling pathway. The integration of human migraine models with advanced imaging and genetic studies will likely continue to yield valuable insights, paving the way for personalized and more effective treatments. Overall, the emerging scientific advances in migraine hold great promise for alleviating the burden of this debilitating condition for the many people afflicted.
Related content

Discover how human models of migraine have identified key molecular triggers like CGRP and PACAP, revolutionizing treatment options and offering hope for patients unresponsive to current therapies.
Migraine affects an estimated 1.1 billions worldwide and ranks as the 2nd leading cause of disability, while being the leading among young adults.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
In human models of migraine, a suspected pharmacological migraine trigger is administered either orally or via infusion to a participant with migraine or a healthy volunteer, typically within a double-blinded, randomized, placebo-controlled design