
Introduction Anxiety Disorders
Anxiety disorders (ANX) collectively represent the most prevalent category of mental illness globally, affecting hundreds of millions of people and imposing a substantial burden on individuals, families, and healthcare systems.1 The group of ANX consists of specific phobias (SP), social anxiety disorder (SAD), panic disorder (PD) with and without agoraphobia (AG), generalized anxiety disorder (GAD), and, considering the lifetime perspective, selective mutism and separation anxiety. The main pathological characteristics of ANX are partly highly burdensome, and prolonged anxiety symptoms in daily life situations can lead to tremendous negative emotional as well as behavioural consequences and individual disability.2 First onset is typically in adolescence (mean age 15 years). Thus, anxiety disorders affect mostly young individuals in important developmental stages, school and professional career and social life.3
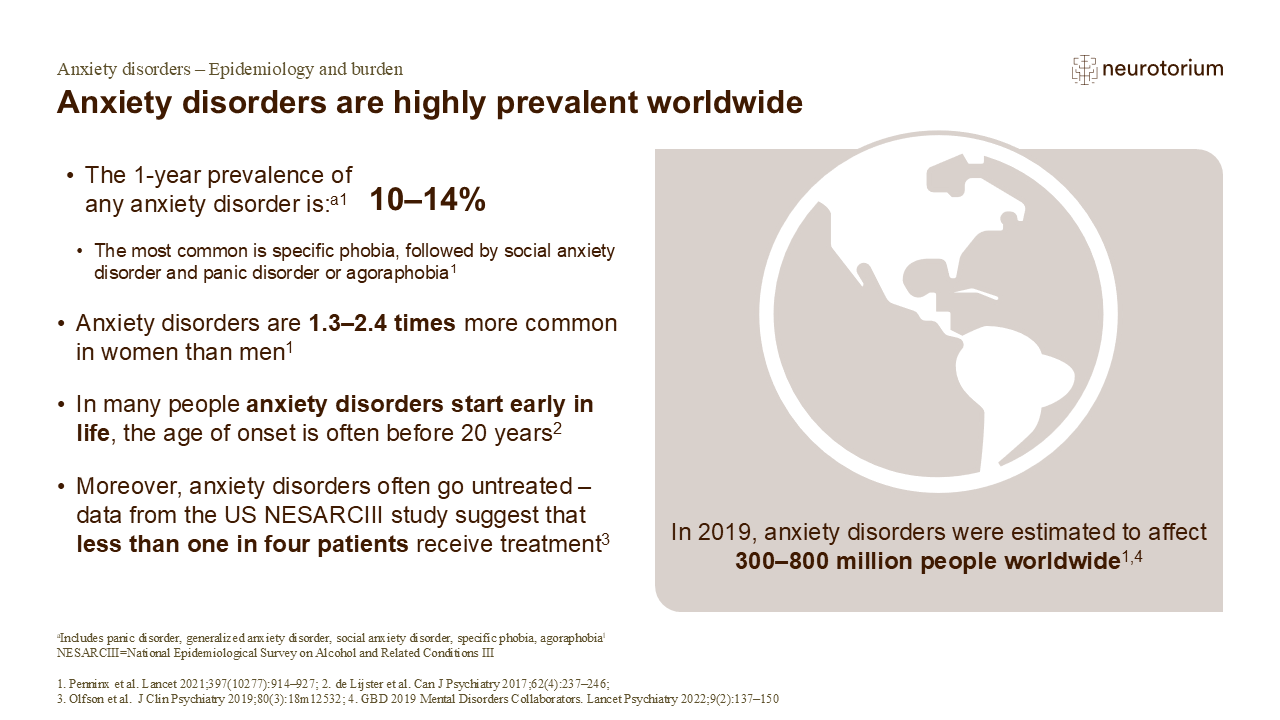
Anxiety disorders are highly prevalent worldwide
Anxiety disorders are among the most common types of mental disorder; however, due to methodological differences, estimates of the prevalence of anxiety disorders in populations around the globe vary widely across large-scale studies.1 During late adolescence and in early adulthood (between 15–25 years of age), the cumulative prevalence of all anxiety disorders is approximately twice that of the 1-year prevalence of 10–14% observed in the adult population.1 While not all anxiety disorders experienced by children and adolescents are severe or requiring medical attention,1 access to treatment is an unmet need among people with anxiety disorders. According to data from the 2012–2013 US National Epidemiological Survey on Alcohol and Related Conditions III (NESARCIII), only 24.1% of patients with anxiety were receiving treatment.3 Treatment rates were highest for panic disorder, followed by generalized anxiety disorder and social anxiety disorder; specific phobias were the least likely to get treated.3
References:
- Penninx BW, Pine DS, Holmes EA, Reif A. Anxiety disorders. Lancet 2021; 397 (10277): 914–927.
- de Lijster JM, Dierckx B, Utens EM, et al. The age of onset of anxiety disorders. Can J Psychiatry 2017; 62 (4): 237–246.
- Olfson M, Blanco C, Wall MM, et al. Treatment of common mental disorders in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions-III. J Clin Psychiatry 2019; 80 (3): 18m12532.
- GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 2022; 9 (2): 137–150.
Anxiety disorders are recognized as complex heritable phenotypes shaped by an intricate interplay of genetic, environmental, and neurobiological factors.4 Understanding the degree to which genetic variation accounts for individual differences in anxiety risk — the disorder’s heritability — and identification of those factors have become a central question in psychiatric genetics.
Heritability of Anxiety Disorders
Decades of twin and family research have established that anxiety disorders run in families and are meaningfully influenced by genetic factors. Family and twin studies suggest an increased recurrence risk of 4-6 times for first degree relatives of patients with ANX to develop any anxiety disorders compared to first relatives of healthy individuals (see Figure 1 for different approaches in genomic studies on anxiety).5 Additionally, a substantial shared genetic component between anxiety disorders drives the risk of first-degree relatives of affected individuals to develop a wide range of pathological anxiety states, e.g. liability to experience panic attacks. High heritability rates mean that genetic variations explain a larger share of why some individuals are more prone to develop an anxiety disorder than others.6 Meta-analyses drawing on twin data report heritability estimates in the range of 30–50% for anxiety disorders, indicating a moderate but consistent heritable component.7,8 However, as these estimates apply to groups, the individual genetic risk to develop a disorder can vary substantially.
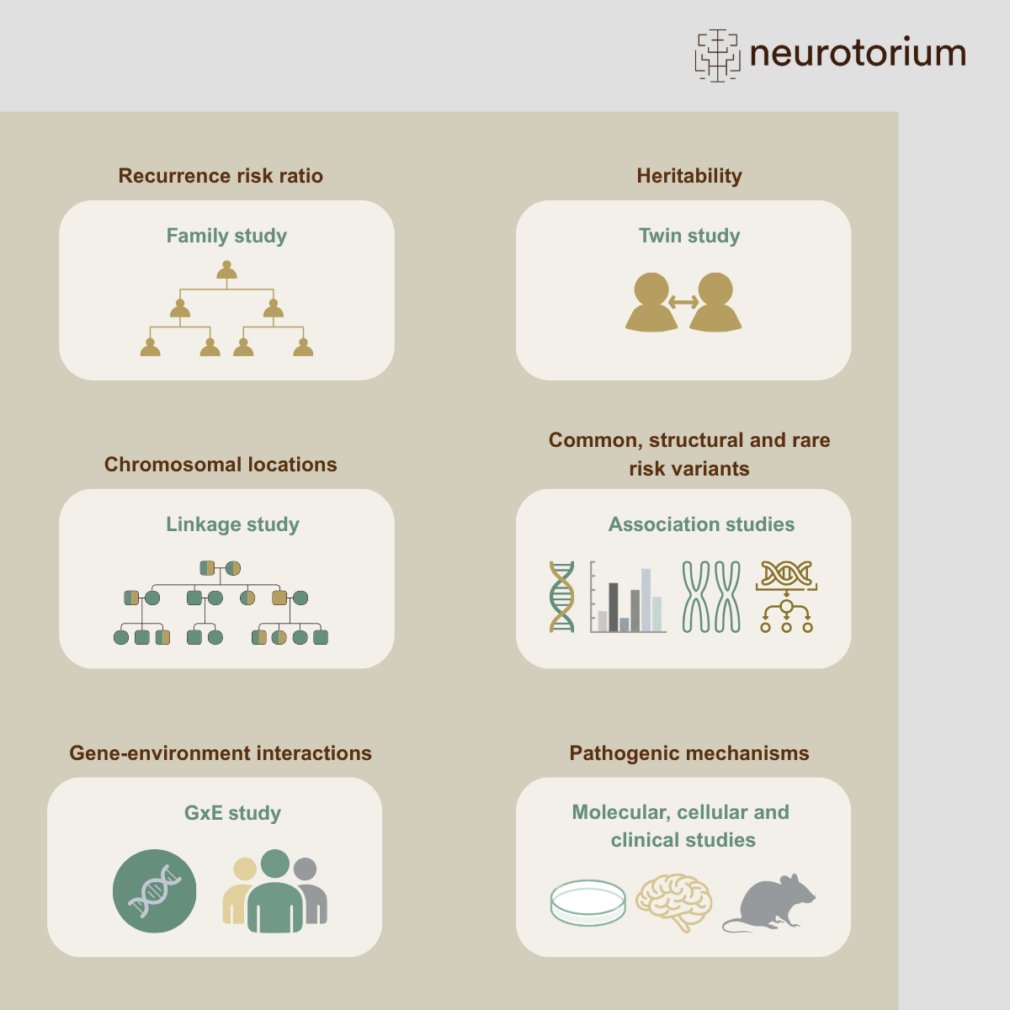
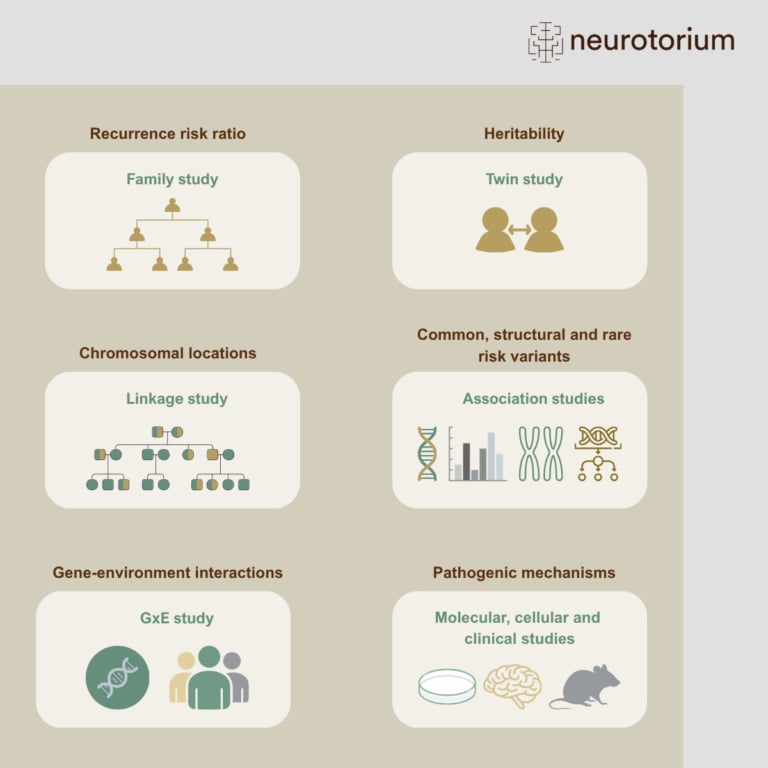
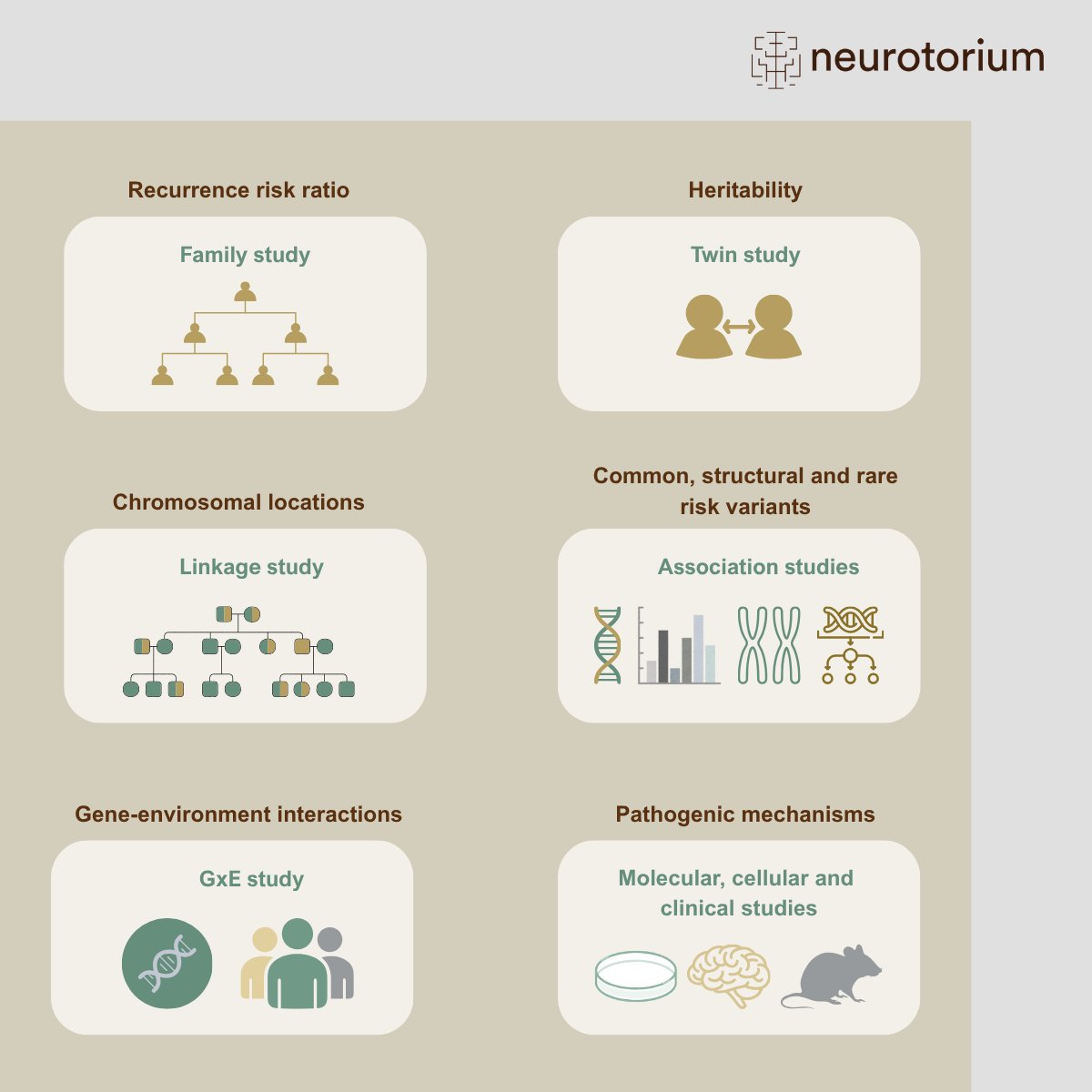
Overview of approaches used to study the genetics of anxiety disorders
Family and twin studies estimate recurrence risk and heritability, showing that anxiety disorders aggregate in families and have a moderate genetic component. Linkage studies identify chromosomal regions that may harbour risk-related genes, while association studies, including genome-wide association studies, investigate common, structural, and rare genetic variants across the genome. Gene-environment interaction studies examine how genetic vulnerability is shaped by environmental exposures, and molecular, cellular, and clinical studies help translate genetic findings into biological mechanisms and potential therapeutic targets.
Genetic studies in anxiety disorders and related traits
Previous evidence strongly suggests a complex and heterogeneous genetic basis in anxiety disorders, including common and rare variants which contribute to the genetic risk with varying degrees of impact and are distributed across the entire genome.9 Most genetic studies in the field of anxiety use linkage and association methodology. Linkage studies compare patterns of genome markers in affected and unaffected relatives within families to find chromosomal locations associated with anxiety rather than pinpointing a single exact mutation. The earlies studies in the field of genetic anxiety research used a linkage approach and identified promising candidate locations and genes for ANX, e.g. related to hormonal stress system regulation (corticotropin-releasing-hormone receptor 1, CRH1), neuropeptide systems (Neuropeptide Y) and neurotransmitter metabolism (COMT).10 However, subsequent replication studies showed limited generalizability of these results to other populations, suggesting that linkage results might be more applicable in highly familial cases.
Beyond linkage studies, genetic association studies examine whether specific genetic variants occur more often in individuals with ANX than in healthy controls (case-control design). The human genome contains several kinds of genetic variations. The most common are single nucleotide polymorphisms (SNPs), where one base is changed at a specific position. In addition, copy number variants (CNVs) denote duplications or deletions of smaller or larger DNA parts. Genetic variants can be common or rare within the population, occurring in a larger or small fraction.
CNVs and rare variants (minor allele frequency < 1%), could occur very recently in families or de novo and can significantly influence the risk of developing a disease. Not many studies so far investigated CNVs in anxiety pathology, most of them suggested that rates of anxiety symptoms are increased in young and adult CNV carriers.11,12 Additionally, Pan et al. (2024) identified association of anxiety symptoms with rare variations in four genes which were related to different functional systems, such as mitochondria and protein-DNA interaction.13 Overall, it must be concluded that the role of rare variants in anxiety disorders still requires further research.
First association studies in anxiety disorders investigated common variants in specific genes of interest (candidate gene studies), which were selected related to their putative function in stress, neurotransmitter systems and fear-related circuits.14 Despite interesting results for single genes (e.g. COMT, CRH1, MAOA, NPSR1), most of the findings could not be replicated, suggesting that other approaches and larger sample sizes are needed to capture the high genetic and phenotypic heterogeneity within anxiety disorders.
Genome-wide association studies (GWAS) simultaneously interrogate a large number of common SNPs across the entire genome in a hypothesis-free approach to identify novel risk variants and genes involved in anxiety disorders. Several large GWAS for various anxiety phenotypes have already been conducted.15-18 Two recent GWAS on Panic disorder were published as preprint.19,20 Naamanka et al. report a significant association of variants in the gene SORCS3 and the levels of SORCS3 protein in the human blood with panic disorder, suggesting that this candidate could potentially serve as a blood biomarker for panic in the future.19 The second study performed a GWAS meta-analyses in panic attacks and panic disorder and resulted in 17 associated variants as well as very similar genetic risk between panic attacks and panic disorder. Interestingly, further analyses revealed high representation of the associated variants not only in the brain neurons but also in neurons of the lung, heart, and eye which suggest a critical role for interoceptive sensory processing and peripheral organ-brain communication in panic pathophysiology, consistent with the hallmark physical symptoms of panic attacks such as altered heart rate and breathing.20 Additionally, one preprint GWAS meta-analysis on anxiety as dimensional measure identified 41 novel locations on the genome, which were functionally related to processes of neuronal communication in the brain.21
The most recent landmark GWAS leveraged data from over 122,000 anxiety disorders cases and 800,000 controls of European ancestry and identified 66 genes and 58 significant risk variants, 51 of which were replicated in an independent sample.22 The follow-up analyses found enrichment in brain regions involved in anxiety-related circuits and pointed to GABAergic signalling as a likely mechanism involved in anxiety risk. GABA (gamma-aminobutyric acid) is one of the main inhibitory neurotransmitters in the brain, so it helps regulate neural firing and dampen overactive fear and stress circuits. As GABA-targeted medication, as benzodiazepines, are potent anxiolytic agents, the study provides converging genomic evidence for a specific role of GABA in anxiety pathology. The genetic architecture of anxiety is also notable for its overlap with other psychiatric conditions. Anxiety shows broad genetic correlations with depression, as well as widespread pleiotropy with several physical health domains.23 Consequently, all the GWAS analyses cited above found substantial genetic correlation between anxiety disorders and depression as well as neuroticism as highly correlated trait phenotypes and other psychiatric disorders, suggesting that these conditions share part of the same genetic architecture.
Despite these advances, a well-documented challenge persists: individual GWAS loci have small effect sizes and collectively explain only a modest fraction of the observed heritability (less than 15% in most of the GWAS on anxiety so far) — a phenomenon termed “missing heritability.”24,25 Emerging evidence suggests that much of this gap may be attributable to gene-regulatory mechanisms, as GWAS hits reside also in non-coding regions, and disruption of gene-regulatory elements may contribute to anxiety disorders by subtly altering neuronal signalling and stress-response pathways.
In addition, both genetic and environmental factors contribute to the onset, development and severity of anxiety disorders with environmental triggers often influencing the expression of underlying genetic risk, also called gene-environment interaction (GxE). GxE interaction occurs when an individual’s genetic makeup influences the sensitivity to environmental exposure, meaning that the same stressor leads to different effects depending on the individual genetic profile. Early life stress, such as childhood maltreatment, abuse and loss of caregivers, is among the most consistently implicated environmental factors with evidence suggesting that specific genetic risk amplify the consequences of early life stress on future anxiety.26 Previous evidence points to transmission of GxE effects by variants in the serotonin-related system and stress system.27,28 Recent research also uses polygenic risk scores, which summarizes the collective genetic risk for anxiety disorders, to investigate how genetic factors interact with a broad range of environmental influences.29 Additionally, mechanisms such as epigenetic modifications represent an important biological pathway how the environment influences gene regulation and subsequent processes in the brain.30,31
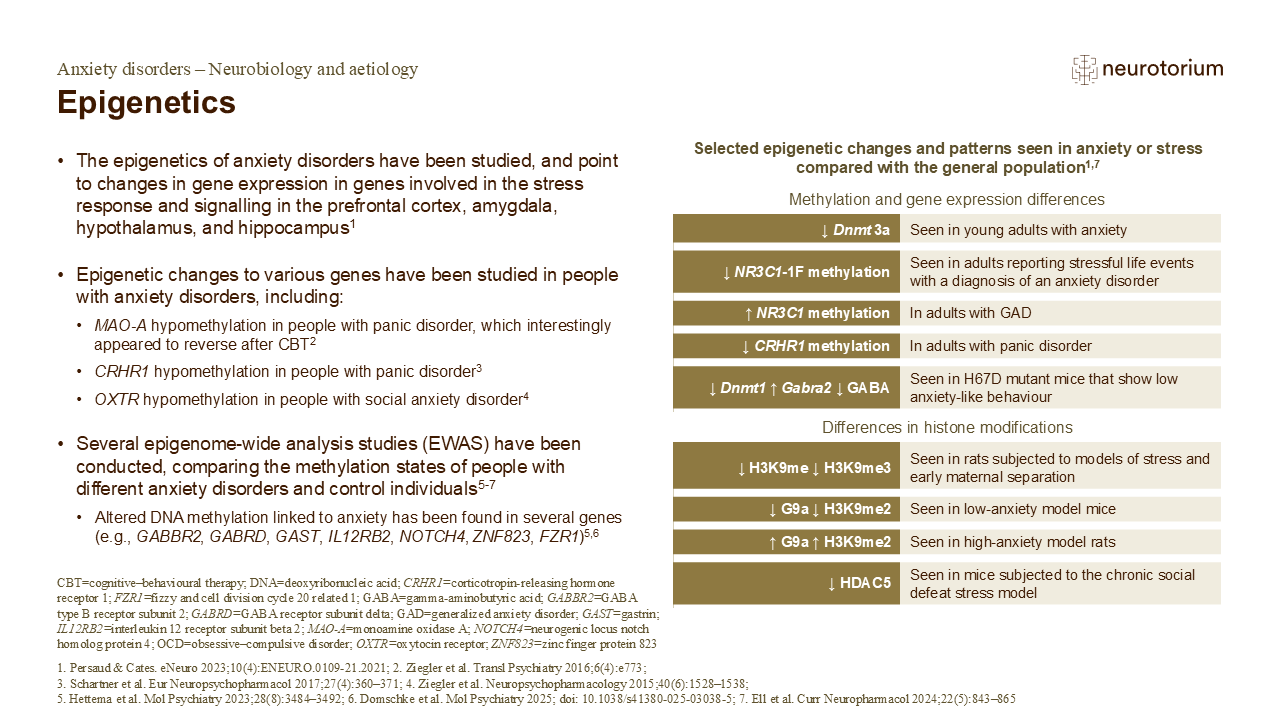
Epigenetics
As outlined in the table on the slide, many differences in gene methylation, expression, and histone modification have been found in either people with anxiety compared with controls, or in animal models of anxiety-like behaviour.1 Happily, some of these experimental observations compliment each other, such as the decreased H3K9me2 marking in a mouse model of low anxiety paired with the increased H3K9me2 marking in a rat model of high anxiety.1
References:
- Persaud NS, Cates HM. The epigenetics of anxiety pathophysiology: a DNA methylation and histone modification focused review. eNeuro 2023; 10 (4): ENEURO.0109-21.2021.
- Ziegler C, Richter J, Mahr M, et al. MAOA gene hypomethylation in panic disorder-reversibility of an epigenetic risk pattern by psychotherapy. Transl Psychiatry 2016; 6 (4): e773.
- Schartner C, Ziegler C, Schiele MA, et al. CRHR1 promoter hypomethylation: an epigenetic readout of panic disorder? Eur Neuropsychopharmacol 2017; 27 (4): 360–371.
- Ziegler C, Dannlowski U, Bräuer D, et al. Oxytocin receptor gene methylation: converging multilevel evidence for a role in social anxiety. Neuropsychopharmacology 2015; 40 (6): 1528–1538.
- Hettema JM, van den Oord EJCG, Zhao M, et al. Methylome-wide association study of anxiety disorders. Mol Psychiatry 2023; 28 (8): 3484–3492.
- Domschke K, Schiele MA, Crespo Salvador Ó, et al. Epigenetic markers of disease risk and psychotherapy response in anxiety disorders – a longitudinal analysis of the DNA methylome. Mol Psychiatry 2025; doi: 10.1038/s41380-025-03038-5.
- Ell MA, Schiele MA, Iovino N, Domschke K. Epigenetics of fear, anxiety and stress – focus on histone modifications. Curr Neuropharmacol 2024; 22 (5): 843–865.
Summary and outlook
Taken together, current evidence positions anxiety disorders as robustly heritable but polygenic conditions whose full genetic underpinnings remain only partially characterised. Recent large GWAS point to a robust implication of GABA-system related genetic factors in anxiety disorders. Continued integration of multi-ancestry GWAS, transcriptomic analyses, and family-based designs will be essential for closing the gap between estimated and explained heritability, and ultimately for translating genetic findings into improved clinical understanding and therapeutic targets.
Related content
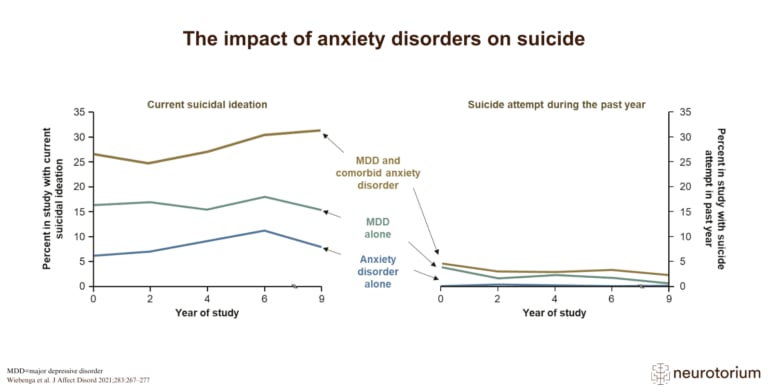
Suicidal ideation is far more common than attempts in people with anxiety or depression, especially with comorbid disorders and severe depression.
{kind=link}